Painful Jerk Test - A Predictor of Success in Nonoperative Treatment of Posteroinferior Instability of the Shoulder
Authors: Kim SH et al.
References: Am J Sports Med. 2004;32:1849-55
Abstract
Background: The jerk test has been used as a diagnostic test of the posteroinferior instability of the shoulder. Pain may or may not be associated with posterior clunking during the jerk test.
Purpose: To evaluate the presence or absence of pain with the jerk test as a predictor of the success of nonoperative treatment for posteroinferior instability of the shoulder and to identify the pathologic lesion responsible for the pain in the jerk test.
Study Design: Retrospective review of prospectively collected data.
Methods: Eighty-one patients (89 shoulders) who had posteroinferior instability with a positive posterior clunk in their shoulders during the jerk test were nonoperatively treated. The patients were divided into 2 groups with respect to the presence of pain in the jerk test: the painless jerk group (54 shoulders) and the painful jerk group (35 shoulders). Response to the nonoperative treatment was evaluated after at least a 6-month rehabilitation program. Patients who did not respond to the rehabilitation underwent arthroscopic examination to identify any pathologic lesions.
Results: The painful jerk group had a higher failure rate with nonoperative treatment (P < .001). In the painless jerk group, 50 shoulders (93%) responded to the rehabilitation program after a mean of 4 months. Four shoulders (7%) were unresponsive to the rehabilitation. In the painful jerk group, 5 shoulders (16%) were successful with the rehabilitation, whereas the other 30 shoulders (84%) failed. All 34 shoulders that were unresponsive to the rehabilitation had a variable degree of posteroinferior labral lesions.
Conclusions: The jerk test is a hallmark for predicting the prognosis of nonoperative treatment for posteroinferior instability. Shoulders with symptomatic posteroinferior instability and a painful jerk test have posteroinferior labral lesions.
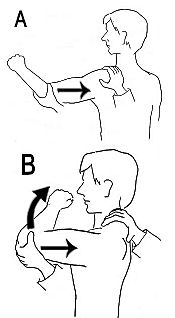
Test Description:
A - An axial force is applied to the arm in 90 degrees of abduction and internal rotation.
B - the patient's arm is horizontally adducted while axial load is maintained.