LARS Ligament Technique
Lennard Funk
LARS Ligament Surgical Technique Corin
</embed />

Incision & Approach
A 3-5cm incision is made in the sagittal plane extending up from the coracoid over the clavicle (blue arrows). Transverse incisions can lead to poor scars.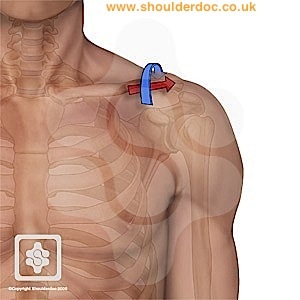
The medial 5cm of the deltoid can be divided off the clavicle and reflected laterally creating a flap for later repair.
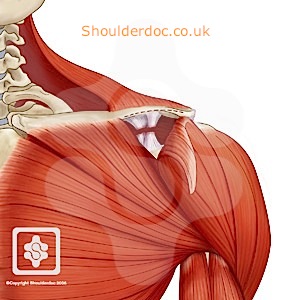
The AC joint and lateral clavicle are then exposed. The coracoid is exposed by blunt dissection.
Preparation
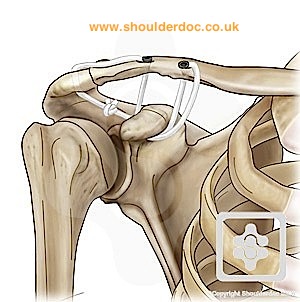
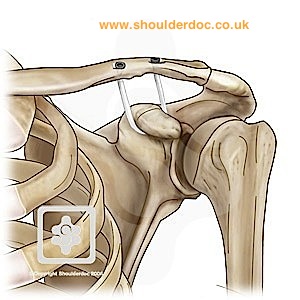
Two oblique drill holes are made in the lateral clavicle, either side of the coracoid. The lateral tunnel is oblique forward and the medial tunnel oblique backwards.
The 3.5 mm drill bit is used for the LAC 20 ligament and the 4.5 mm drill for the LAC 30 CK.
When the drilling the tunnels, place a retractor on the inferior aspect of the clavicle, to prevent any damage when the drill bit exits.
Ensure that the drill bit is central on the bone so as to not damage the anterior and postererior cortices.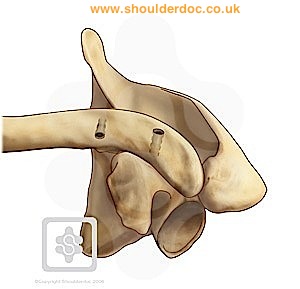
The wire guide, with a loaded wire, is passed medially under the coracoid, from medial to lateral. 

Expose the end of the wire passer and set up the wire-passer cannula. Turn it several times to get the top of the hook free from the fibrous tissues which may be interposed. Insert the drift to complete the free passage for the wire loop.
Push the wire loop through whilst removing the cannula. 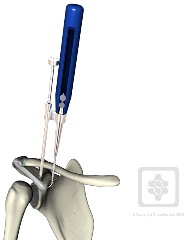
Load the ligament in the wire loop and pull the guide through and out, thus passing the ligament around the coracoid.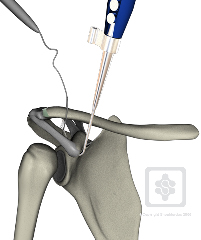
The ligament is passed under the coracoid, by pulling on the wire guide as it is removed from under the coracoid. 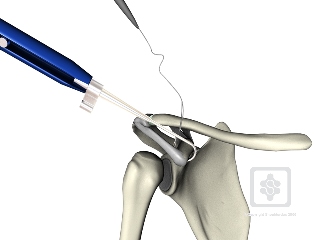
Wire loops are passed through the clavicular tunnels, pulling the ligament through each tunnel.
Tension is created by pulling alternately on each side, whilst holding the reduction of the AC joint.
We like to use a bone reduction forceps to assist with the reduction, with one side under the coracoid and the other over the lateral clavicle.
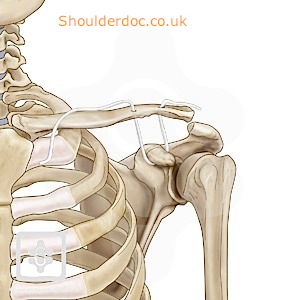
The ligament ends are fixed in the bony tunnels with titanium interference screws. The two diameter screws available are 4.7 x 15 mm or 5.2 x 15 mm.
Use the 4.7 screw for the LAC 20 ligament and the 5.2 screw for the LAC 30.
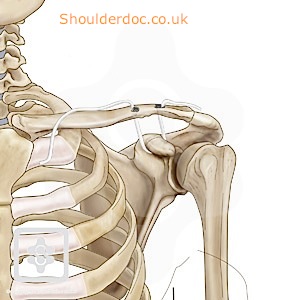
The ends of the ligament are cut flush to the superior aspect of the clavicle, leaving no troublesome projections.
The reduction is confirmed by assessing the height and translation in relation to the acromion.
The incision is closed by suturing together the trapezo-deltoid fascia and reattaching the lateral deltoid.
Post-operative x-rays: 
Wound at 6 weeks:
Modifications
"We have modified the technique to further strengthen the repair in two ways:
1. By passing the excess ligament around the coracoid again and then
tying it sub-deltoid in a figure-of-eight configuration
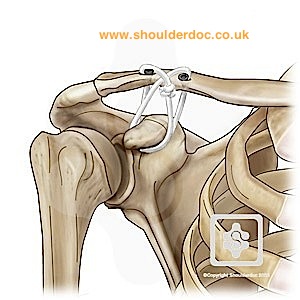
2. By passing the excess lateral ligament through another 3.5mm
oblique drill hole in the acromion and then back to the medial
ligament passed under the coracoid again. This recreates the
acromio-clavicular ligaments, as well as the coraco-clavicular
ligaments and is used for revision cases."