MR Arthrogram and Arthroscopy of the Shoulder: A Comparative Retrospective Study with emphasis on Posterior Labral lesions and Radiologist Locality.
Authors: N Karson, J Geoghan, L Funk
References: European Shoulder & Elbow Society Meeting, Lyon - 13-16 September 2011
Background: Magnetic resonance arthrography (MRA) is a routine diagnostic investigation for glenohumeral lesions, however diagnostic arthroscopy remains the gold standard.
Aim: To investigate the diagnostic accuracy of glenohumeral MRA compared to arthroscopy, with particular interest in previously unreported aspects, such as posterior labral lesions and the locality of the reporting radiologists.
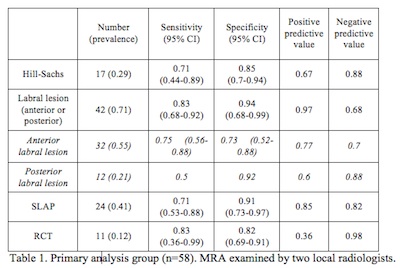
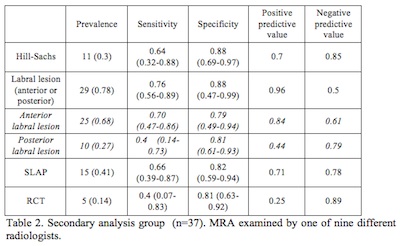
Methods: Ninety-five consecutive patients with pre-operative MRA and subsequent arthroscopy were included. Patients were grouped into MRA reported by specialist radiologists within the specialist shoulder unit (n=58) or reported by non-local musculoskeletal radiologists (n=37).
Results: In the local radiologist group the sensitivity/specificity for Hill-Sachs lesions was 0.71/0.85, anterior labral tears 0.75/0.73, posterior labral tears 0.50/0.92, SLAP lesions 0.71/0/91 and rotator cuff tears (RCT) 0.40/0.81. In the non-local radiologist group the sensitivity/specificity for Hill-Sachs lesions was 0.64/0.88, anterior labral tears 0.70/0.79, posterior labral tears 0.40/0.81, SLAP lesions 0.66/0/82 and RCT 0.40/0.81.
Sensitivity/specificity was lower for lesions reviewed by the non-local radiologists.
Discussion: MRA is not 100% sensitive or specific and does not negate arthroscopy. There is a lower diagnostic accuracy of posterior than anterior labral lesions and improved accuracy of glenohumeral MRA diagnosis may be achieved with increased experience of radiologist within specialist units and regular surgical feedback of cases.
Additional Comments from study:
- Differences between local- and non-local MRA data suggest that diagnostic accuracy is better when surgeon and radiologist work closely together.
- One in five patients with labral pathology will be missed on MRA.
- 19/24 anterior and 6/12 posterior tears were correctly identified on MRA. Analysis of anterior and posterior labral lesions separately revealed that whilst MRA was sensitive for the presence of a labral tear, its ability to accurately determine the location of the lesion was low.
- Negative scan results are not absolute and should not preclude investigation with arthroscopy
- Improved results from the local radiologists hints that best results are obtained when a feedback loop between surgeon and radiologist is available.
- The accuracy of MRA to determine the location of a labral tear was low