
Pectoralis Major Rupture
Lennard Funk
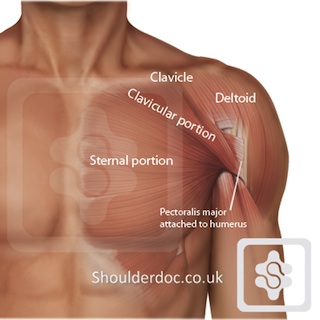
The Pectoralis major is a very powerful muscle that forms the chest prominence and. It moves the shoulder forwards and across your chest. It is best known as the muscle that you develope with the bench press exercise.
The pec major attaches to the humerus bone (upper bone of arm) and is divided into two parts. The upper part is known as the 'clavicular head' and the lower part the 'sternal head', based on their origins from the clavicle and sternal bones repsectively.
Ruptures of the pectoralis major muscle are becoming more common due to the increase in power sports weight training. It most commonly occurs during bench pressing and is felt as a painful snap at the front of the shoulder and chest. The muscle then 'bunches up' and deforms. Bruising and swelling is common.

Left pec major rupture. Note bruising and asymmetrical chest
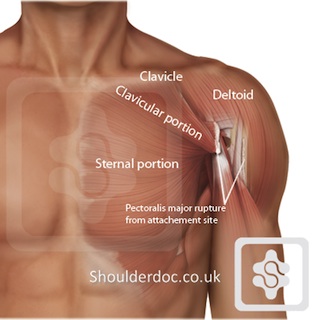
Rupture of the sternal and clavicular parts of the Pec Major, with the muscle retracted, giving the 'bunched-up' appearance on the outside
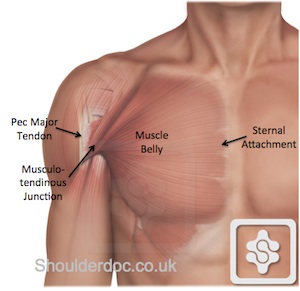
The Pectoralis major may tear/rupture in the following parts of the muscle:
- Tendon rupture off the humerus bone (most common)
- Tear at the junction of the muscle and tendon (musculo-tendinous junction)
- Tear within the muscle belly itself
- Muscle tearing off the sternum (very rare)
Treatment:
The pec major muscle is not essential for normal daily shoulder function, but is important for srenuous activities. Patients who wish to return to active athletic and manual activities are likely to benefit from surgical repair.
A large statistical review (meta-analysis) of 112 cases of pectoralis major rupture, patients who undergo surgical repair had less pain, a higher rate of pre-injury strength and return to activities, than patients managed conservatively [Bak et al.]. Outcome studies comparing conservative with surgical
treatment have demonstrated that surgically repaired injuries regained 97% of the strength of the uninjured arm vs. 56% in non-operative patients [Hanna et al.]
The earlier a repair is performed the easier the surgery. Small studies have shown that the outcomes after early primary repair have generally been superior to those of delayed repair [Aarimaa et al. and Bak et al]. My own results showed no difference in outcomes between early and delayed direct repairs. [Shah et al. TSES, 2009].
However, it is important to bear in mind that this is an uncommon injury and the literature is based largely on case reports, small series, and systematic reviews of these small series. There is a lack of high-quality good evidence for surgical versus non-surgical management and early versus delayed repairs. Outcomes in the literature are also presented heterogeneously, so it is difficult to compare them.
Where the tear cannot be directly repaired (i.e. massive, involving musculo-tendinous tissue or chronic) reconstruction can be considered. This is done using a tendon graft. I have found Achilles Tendon Allograft to be the strongest and most reliable tendon graft, and used this reliably since 2004. For information on tendon allografts click here.
The decision on which pec major tears to repair and when depends on the type of tear, how old it is, how retracted it is, the demands and requirements of the patient and the expertise of the surgeon.
The common types I see are:
Acute (< 3 months)
- Tendon avulsion = repair as soon as possible directly to the bone
- Musculo-tendinous tear = I prefer to wait for consolidation of the scar tissue and then reef the muscle-tendon junction with a special high strength suture material that encourages healing (Orthocord). (you cannot repair muscle directly, therefore wait for some fibrous tissue either side of the tear)
- Muscle tear = extremely rare and almost impossible to repair, but can do as above and reinforce with achilles tendon allograft.
Chronic (> approx. 3 months):
- Tendon avulsion - if retracted lateral to nippple line usually can still do a direct repair; if retracted medial to nipple line needs a tendo-achilles allograft reconstruction
- Musculo-tendinous & muscle tear - reef repair using high strength biological suture, like a hernia repair.
Outcomes of Surgery:
| Injury | Technique |
Improvement in
Cramping Pain |
Improvement in Press Strength
|
Improvement in Cosmesis
|
| Tendon Avulsion (Acute) |
Direct Repair | 80% | 90% | 80% |
| Tendon Avulsion (Chronic) |
Direct Repair | 80% | 90% | 70% |
| Tendon Avulsion (Chronic) |
Allograft | 50% | 70% | <10% |
| Musculotendon Tear (> 6wks) |
Direct Repair | 75% | 75% | 50% |
| Musculotendon Tear (> 6wks) |
Auto/Allograft | 50% | 50% | <10% |
Complications of Pec Major Surgery
- Deep infection = 10%
- Superficial infection = 10%
- Post-op stiffness at 3 months = 12%
- Rerupture rate = 20% overall (higher with allograft and revisions)
- Haematoma/bleeding = 2%
Surgery for Pec Major Tear
For more information on the surgery click here (please note that the page includes surgical photographs, which may offend some viewers)
 Related Articles
Related Articles
Also See:
