
T4 Syndrome
Eleanor Richardson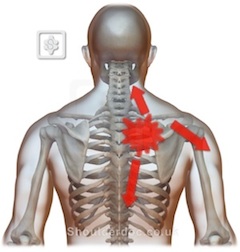
What is it?
T4 syndrome, or more accurately “upper thoracic syndrome”, is a rare and perhaps under-recognized clinical entity that warrants attention. Upper thoracic syndrome is based on the premise that dysfunction of the joints in the thoracic spine (including the intervertebral/zygaphophseal, costovertebral and costotransvere joints) can refer pain and paraesthesia to the upper limbs and the hands. As sympathetic outflow to the upper limb is supplied by levels T2-5, the sympathetic nervous system could provide a pathway for referral from the thoracic spine to the upper limb. This syndrome is 3 times more common in women than men.Although this syndrome is poorly defined in the literature, the cluster of symptoms reported in T4/Upper thoracic syndrome include:
- Subjective reports of parasthesia, altered and extreme temperature perception and “puffiness” in the glove distribution of both hands
- A history, or current complaint of intermittent posterior thoracic pain or pain around the scapula region
- Symptoms worse last thing at night or with activities involving thoracic flexion/slumping (e.g sitting at a computer/desk for long periods, laying with pillows under your head)
- Position of most comfort tends to be laying completely flat (supine)
Objective assessment findings include:
- Increased cervical lordosis and cervico-thoracic kyphosis
- Flattened upper thoracic spine (T2-7)
- Minimal thoracic movement during single arm elevation to either side
- Notable restriction in upper thoracic movement
- Local tenderness and symptoms reproduced with mobilisation of the spine anywhere between levels T2-7 (historically including T4)
- Local hypomobility of the vertebral segment associated with symptoms
- Positive upper limb tension tests, often limited on both sides by pain across upper thoracic spine
- Positive slump test
How is it Diagnosed?
In the absence of a gold standard for diagnosing this poorly understood condition, the patient’s symptomatology coupled with the ability to elicit/reproduce comparable symptoms with manipulation over the relevant thoracic spinal level forms the basis of this clinical diagnosis. Pain provocation with palpation has been advocated as a reliable means for identifying symptomatic structures in T4 syndrome and is an important factor in clinical decision making. Symptoms that do not appear wholly somatic in origin or those which are likely to be sympathetically maintained also provides clues towards the diagnosis (for example, a non dermatomal referral and pain patterns). Poor responses to muscle relaxants, absence of an inflammatory pain pattern and a clear association between a patient’s movement impairment and their clinical symptoms are also important considerations in this clinical diagnosis.Imaging studies are of no use in patients whose symptoms are sympathetically maintained and driven by thoracic dysfunction, however they do play an important role in ruling out other pathologies that may be mimicking this clinical condition.
What are the possible Differential Diagnosis that need to be ruled out?
The following conditions should be ruled out either during the subjective history taking, objective assessment or through the use of appropriate imaging studies:
- TOS (vascular, true neurological or symptomatic)
- Carpal Tunnel Syndrome
- Cervical/Thoracic radiculopathy/disc disease
- Vascular disease (consider spinal stenosis)
- Neurological disease (e.g. MS)
- Multiple level space occupying lesions
- Zygaphophseal joint artrhopathy
- Ankylosing spondylitis
- Myogenic causes (trigger points, muscle strains)
- Vertebral or rib fracture
- Diffuse idiopathic skeletal hyperostosis (DISH)
- Intercostal neuralgia
- Visceral sources/drivers including cancer, cardiac, pulmonary, gall bladder, hepatobiliary, renal and gastroesophageal conditions as these can all cause referral to the thoracic or scapular regions
What is the Treatment for T4 Syndrome?
Physiotherapy is crucial in the management of this clinical entity and this will involve an experienced physiotherapist applying an impairment based approach to manual therapy in combination with a home exercise programme consisting of localised thoracic exercises targeted at the movement dysfunction found at the relevant motion segments in the spine. Postural control exercises along with range of motion exercises will also play an important part in your rehabilitation. As treatment moves forward your therapist should progress any manual therapy or exercise regimes into more functionally relevant positions (for example sports/work/activity specific). With adherence to both physiotherapy and home exercises full resolution of your symptoms is highly likely but your therapist will discuss your individual realistic outcomes and goals at each stage of your rehabilitation.References
- Bialosky, J. E., Bishop, M. D., Price, D. D., Robinson, M. E., and George, S. Z. (2009) The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Manual Therapy, Vol. 14, pp. 531-538
- Bodduk, N. (2002) Innervation and pain patterns of the thoracic spine. In: Physical therapy of the cervical and thoracic spine ed Grant R. Clinics in Physical Therapy, Vol. 17, 3rd ed, Churchill Livingstone, pp. 73-81
- Conroy, J. L., and Scneiders, A. G. (2005) The T4 syndrome. Manual Therapy, Vol 10, no. 4, pp. 292-296
- Crawford, H.J., and Jull, G.A, (1993) The influence of thoracic posture and movement on range of arm elevation. Physiotherapy, Vol. 9, pp. 143-148
- Edmondson, S. J., and Singer, K. P. (1997) Thoracic spine: anatomical and biomechanical considerations for manual therapy. Manual Therapy, Vol, 2, no. 3, pp. 132-143
- Evans, P. (1997) The T4 syndrome: some basic science aspects. Physiotherapy, Vol. 83, no. 4, pp.187-189
- Fruth, S.J. (2006) Differential diagnosis and treatment in a patient with posterior upper thoracic pain. Physical Therapy, Vol. 86, no. 2., pp. 254-268
- Maitland, G., Hengeveld, E., Banks, K. and England, K. (2005) Maitland’s vertebrall manipulation. 7th ed. Edinburgh: Butterworth Heinemann
- Jowsey, P., and Perry, J. (2010) Sympathetic nervous system effects in the hands following a grade III poster-anterior rotatory mobilisation technique to T4: a randomised control trial. Manual Therapy, Vol. 15, pp. 248-253
- Watson, L. A., Pizzari, T., and Balster. S. (2009) Thoracic outlet syndrome part 1: clinical manifestations, differentiation and treatment pathways. Manual Therapy, Vol. 14, pp. 586-595
