
Superior Capsular Reconstruction (SCR) for Clinicians
Arthroscopic Superior Capsular Reconstruction for irreparable rotator cuff tears
Phoebe Linton & Lennard Funk, 2015
Massive rotator cuff tears are defined as tears that are larger than 5cm, and involve both the supraspinatus and infraspinatus muscle. They continue to pose problems to physicians as being one of the largest pathological shoulder conditions currently. The prevalence of rotator cuff tears increases with age – with 4% of asymptomatic patients aged less than 40 years and 54% of patients aged 60 years or over, having partial or complete tears of the rotator cuff on MRI scanning[1] It has been shown that tears occur due to degeneration of the rotator cuff – this may be genetic or simply ‘wear and tear’. Trauma such as a fall may cause a tear, this is usually in combination with pre-existing degeneration of the rotator cuff[2].
Although many rotator cuff tears can be repaired with excellent results, chronic massive tears of the rotator cuff are a continuing problem to treat. These are what can be described as ‘irreparable’ rotator cuff tears – where the torn tendon cannot reach to the original footprint on the humerus. This is due to tendon retraction with inelasticity, muscle atrophy and fatty infiltration. Currently, there are limited options for patients with irreparable rotator cuff tears but prolonged conservative treatment can have negative effects and lead to further degeneration of the rotator cuff[3]. Patch graft surgery is sometimes carried out, where one of various materials have been sewn to the torn tendon[4]. However, this is associated with a high re-tear rate. A reverse total shoulder arthroplasty is also an option, but this is high risk and leaves no further options should it fail, not to mention the fact that it’s a major procedure especially for younger patients[5]. Along with the development of the SCR by Dr Teruhisa Mihata in 2007, comes potential new hope for patients who have previously been told their rotator cuff is irreparable.
The longer a tear goes without being remedied, the more the tendon and muscle atrophies to fat. Rotator cuff tears cause increased superior translation therefore causing subacromial impingement. This is often what causes the pain that patients with a rotator cuff tear will present with.
Options do exist for massive rotator cuff tears such as debridement and subacromial decompression, partial repair, transposition of the subscapularis tendon, transplantation of the teres major muscle, supraspinatus muscle advancement, deltoid flap reconstruction, latissimus dorsi transfer, pectoralis major transfer, grafting to the torn tendon, and reverse total shoulder arthroplasty. However, it has been proven that any alternative to complete repair is inferior with regards to post-operative complications and clinical outcome[6].
A reverse total shoulder arthroplasty is usually only performed in elderly patients, possibly as a last resort. It is a large operation and comes with known complications – infection, failure, fracture and neurovascular problems. Not to mention the fact that there are no viable options should it fail[7]. Patch graft surgery is commonly used and does have good outcomes, especially in relation to pain relief. Various materials have been reported to have been used as the patch, such as porcine small intestinal submucosa, porcine dermal collagen, and allografts. This surgery involves grafting to the torn tendon to reconstruct the supraspinatus tendon[8][9].This surgery comes with a high re-tear rate[6]– to understand why this occurs so often we have to look at the role of the superior capsule of the rotator cuff.
Although it is well known that the shoulder capsule has a large role in stabilising the rotator cuff, the superior portion of this capsule was relatively un-researched until recently. The superior shoulder capsule is a thin membranous structure[10],[11],[12] that is attached to a large area of the greater tuberosity (between 30% and 61%)[2]and massive tears of the rotator cuff lead to complete defects of the superior capsule. Ishihara et al hypothesised that a large defect in this will significantly increase glenohumeral joint translation, rotational range of motion and subacromial contact pressure. In this study, 7 cadaveric shoulders were used to simulate both a tear in the superior capsule, and a complete defect. The results were conclusive – the superior shoulder capsule plays an important role in passive stability of the glenohumeral joint. A tear in the superior capsule, increased glenohumeral translation in the anterior and inferior directions whereas a defect in the capsule increased glenohumeral direction in all directions, as well as increasing subacromial contact pressure and rotational range of movement[13].This leads to increased laxity of the shoulder joint and consequently increased risk of secondary shoulder arthropathy[13][14].
Perhaps this study explains the reasoning behind why the re-tear rate of patch graft surgery is so high – the lack of superior stability causes subacromial impingement which leads to abrasion of the graft and subsequently a re-tear. I believe it is the reconstruction of the superior capsule, and consequently, stabilisation of the glenohumeral joint, that leads to such a high success rate following the superior capsular reconstruction, in terms of function, pain relief, and post-operative complications.
The SCR was pioneered by Dr Teruhisa Mihata in 2007, and is becoming increasingly accepted in the surgical field. He recently published a follow up paper regarding 24 of his patients with very successful results – showing improvements in American Shoulder and Elbow Score (ASES), acromiohumeral distance as well as pain relief[6].
The SCR involves using a fascia lata autograft, an Arthrex allograft or a Graftjacket Maxforce. An advantage of the SCR is that it can be performed both openly and arthroscopically, with the patient either in the lateral decubitus position or the “beach-chair” position. The arm should be maintained comfortably by the patient’s side (neutral abduction) and in neutral rotation. Any associated lesions should be remedied before the graft is fitted as to aid in balancing the normal force couples of the shoulder. The supraspinatus and infraspinatus should be repaired as much as possible, a biceps tenotomy or tendonesis should be performed on any bicep tear or instability and the superior glenoid and greater tuberosity should be debrided to prepare for reconstruction. Using suture anchors, the graft is attached medially to the glenoid superior tubercle and laterally to the greater tuberosity. Side-to-side sutures between the graft and the infraspinatus tendon, as well as between the graft and the residual anterior supraspinatus/subscapularis can also be added to improve force coupling[6].
The first trial of SCR shows very promising results – Mihata tested 24 shoulders in 23 patients with large to massive irreparable tears. Acromiohumeral distance increased from 4.6 ±2.2mm pre-operatively to 8.7 ±2.6mm post-operatively, mean active elevation increased from 74° to 148° and the ASES increased from 23.5 to 92.9. In this study, there were no complications such as neural injury, infection or suture anchor problems, and there were no re-tears in 20 of the 24 shoulders during the follow up period (24-51 months)[6].
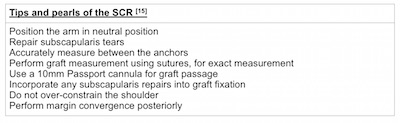
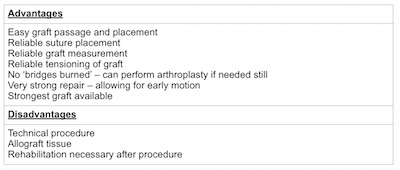
There is continuing research and debate surrounding what the most efficient, reliable material is to use to reconstruct the capsule. In Dr Mihata’s original study, a fascia lata autograft from the patient’s thigh was proposed to use as a graft for the SCR – measured and folded over to create a thick superior capsule imitation. However, studies have recently shown that using an Arthrex dermal allograft may be a better choice – it demonstrated maximum loads 2.5 times greater than the fascia lata autograft[16]. Hirahira et al also published what they believed to be an improved technique on the original, they used an allograft, negating the need for the fascia lata autograft. They concluded that this technique allowed for faster mobilisation postoperatively and for a more accurate measurement and placement of the graft[15].
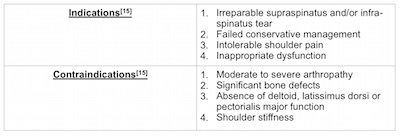
With rotator cuff pathology making up between 30% and 71% of the reasoning behind presenting shoulder complaints to clinicians [17], there is always room for development of treatment. In the appropriate patient, the SCR is a promising alternative to other more hazardous surgical procedures that may end up delaying adequate treatment of massive tears. Biomechanical studies surrounding the superior capsule have provided invaluable evidence supporting the mechanism behind the SCR and several case series corroborate the results published by Mihata in 2014. The vital concept is that the rotator cuff is only the dynamic stabiliser of the shoulder; the superior capsule maintains static stability and is the main constraint against glenohumeral translation. This explains why the SCR can provide pain relief and improve function, without having to perform a salvage repair on the torn tendon. Long term results are yet to be established, and research is still ongoing with regards to optimal technique, but the SCR is proving to be an exciting new development in rotator cuff tear treatment with statistically significant positive results.
Presentation describing the history, biomechanics, and technique for the superior capsular reconstruction for massive, irreparable rotator cuff tears:
Surgical Technique for SCR:
References:
- Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg Am. 1995;77(1):10-15
- Matthews TJW, Hand GC, Rees JL, Athanasou NA, Carr AJ. Pathology of the torn rotator cuff tendon – Reduction in potential for repair as tear size increases. The Bone and Joint Journal. 2006;10.1302/0301
- Ellman H, Hanker G, Bayer M. Repair of the rotator cuff: end-result study of factors influencing reconstruction. J Bone Joint Surg (Am) 1986;68-A:1136-44
- Mori D, Funakoshi N, Yamashita F. Arthroscopic surgery of irreparable large or massive rotator cuff tears with low grade fatty degeneration of the infraspinatus: Patch autograft procedure versus partial repair procedure. Athroscopy 2013;29:1911-1921
- Saltzman BM, Chalmers PN, Gupta AK, Romeo AA, Nicholson GP. Complication rates comparing primary with revision reverse total shoulder arthroplasty. J Shoulder Elbow Surg 2014;23:1647-1654
- Mihata T, Lee T, Watanabe C, Fukunishi K, Ohue M, Tsujimara T, et al. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy 2013;29:459-70. http://dx.doi.org/10/1016/j.arthro.2012.10.022
- Farshad M, Gerber C. Reverse total shoulder arthroplasty – from the most to the least common complication. Int Orthop 2010;34:1075-1082
- Ozaki J, Fujimoto S, Masahura K, Tamai S, Yoshimoto S. Reconstruction of chronic massive rotator cuff tears with synthetic materials. Clin Orthop Relat Res 1986;173-183
- Heikel HV. Rupture of the rotator cuff of the shoulder. Experiences of surgical treatment. Acta Orthop Scand 1968;39:477-492
- Clark JM, Harryman DT 2nd. Tendons, ligaments, and capsule of the rotator cuff. Gross and microscopic anatomy. J Bone Joint Surg Am 1992;74;713-25
- Nimura A, Kato A, Yamaguchi K, Mochizuki T, Okawa A, Sugaya H, et al. The superior capsule of the shoulder joint complements the insertion of the rotator cuff. J Shoulder Elbow Surg 2012;21:86-72
- Clark J, Sidles JA, Matsen FA. The relationship of the glenohumeral joint capsule to the rotator cuff. Clin Orthop Relat Res 1990;254;29-34
- Ishihara Y, Mihata T, Tamboli M, Nguyen L, Jin Park K, McGarry MH, Takai S, Lee TQ. Role of the superior shoulder capsule in passive stability of the glenohumeral joint. J Shoulder Elbow Surg 2014 23;642-648
- Neer CS, 2nd. Craig EV, Fukuda H. Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-44
- Hirahira AM, Adams CR. Arthroscopic Superior Capsular Reconstruction for Treatment of Massive Irreparable Rotator Cuff Tears. Arthroscopy Techniques, 2015;4.6;e637-e741
- Liebler S. Biomechanical testing of Arthrex Allograft vs. Fascia lata autograft as a suitable medium for superior capsular reconstruction. 2015;16.2;p8
- Matsen FA, Titelman RM, Lippit SB, Wirth MA, Rockwood CA. Rotator cuff. In the Shoulder. 2004;3;695-790
