
Nerves about the Shoulder
Axillary Nerve
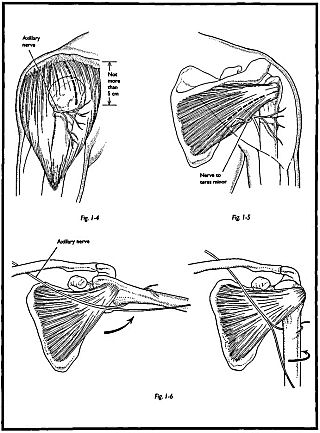
The axillary nerve is the most commonly injured nerve in shoulder surgery. It is in most danger where it passes on the inferior aspect of the shoulder joint capsule. Abduction and internal rotation appose the nerve to the inferior capsule. Adduction and external rotation is safer (Figs. 1-4 to 1-6). Also, it lies near the medial margin of the subscapularis muscle and may be cut during anterior shoulder approaches unless dissection is performed under direct vision. The axillary nerve is also in danger, because it lies on the deep surface of the deltoid after passing round the neck of the humerus. Any incision that relies on splitting of deltoid beyond 5 cm from the tip of the acromion may cause danger to the axillary nerve and can possibly denervate the anterior two thirds of the deltoid.
Musculocutaneous Nerve
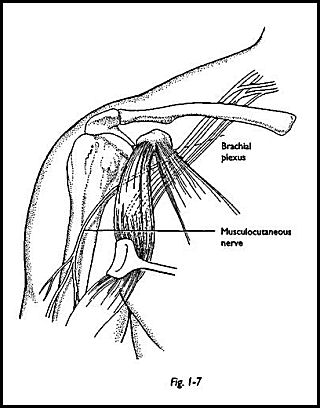
The musculocutaneous nerve passes 2 to 9 cm below the tip of the coracoid and may be endangered by surgery around the tip of the coracoid process. It may become trapped in transfer of the coracoid process or reflection of the conjoined tendon. It is a good general principle not to detach the tip of the coracoid process with its attached muscles when doing the standard anterior approach to the shoulder, because if this is retracted distally, a traction lesion of the musculocutaneous nerve is easily sustained (Fig. 1-7).
Accessory Nerve
The accessory nerve is prone to damage during neck surgery because of its relatively superficial position in the posterior triangle of the neck.
Suprascapular Nerve
The suprascapular nerve is fairly rigidly held at the superior aspect of the scapula by the transverse scapular ligament as it crosses the suprascapular notch and as it wraps round the neck of the spine of the scapula. In this position on the back of the glenoid neck, the nerve is in maximum danger when the shoulder is approached posteriorly. Unfortunately, the incidence of suprascapular nerve injury is increasing with arthroscopic stabilization of the shoulder, which employs blind tying of knots on the posterior aspect of the glenoid neck.
