
Acromial Epiphysiodesis
Indications
The indications for acromial epiphysiodesis appear to fall into two main groups, the athlete and patients with a cuff tear.
Athletes
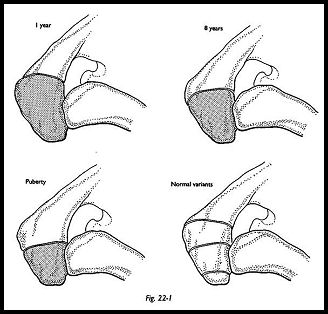
Acromial epiphysiodesis is indicated for the young athlete with pain arising from the unfused epiphysis that is due to excess activity, such as martial arts and fencing. The mechanism of pain is similar to that of Osgood-Schlatter's disease in the tibial tuberosity. Usually, the condition improves with explanation and rest. Some top-level athletes, however, may persist with symptoms and may require fusion of the epiphysis. It is known that in 7 percent of the population the anterior acromion may remain unfused after the age of 30 years (Fig. 22-1).
CuffTear
When the unfused epiphysis is seen in association with a rotator cuff tear, it is usually movable and flail. If the unfused segment is small and very anterior, this may safely be removed as part of the anterior acromioplasry procedure to decompress when repairing the cuff tear. If the segment is larger, however, involving the anterior half of the acromion, then excision is impossible; it would completely disinsert the deltoid and give rise to the problems associated with the old-fashioned radical acromionectomy.
Preoperative Investigation
The axillary view radiograph shows clearly the unfused epiphysis and aids in the decision to (1) excise the small anterior unfused epiphysis or (2) internally fix and fuse a larger segment. Athletes are clinically locally tender to pressure over the epiphysis, which can be reheved by local anesthetic. This may be associated with swelling after sport. In the cuff tear group, subacromial injection and the compression test will confirm that the symptoms are due to impingement. The rotator cuff tear -will have to be repaired, but the epiphysial fusion will have to be done at the same time if the segment is flail.
Technique
Small Unfused Acromial Segment
A small anterior segment may be excised by sharp dissection, staying very close to bone and preserving the tendinous origin of the deltoid. At the undersurface, the remaining acromium can be chamfered to eliminate overhang and then the tendinous stump can be sutured directly to drill holes in the acromium.
Large Unstable Acromion
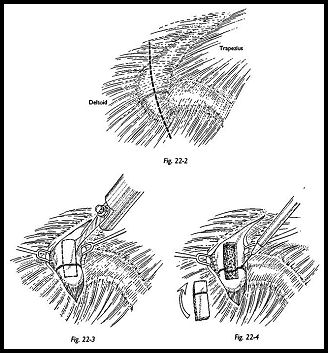
Epiphysiodesis is required to prevent continuing impingement following rotator cuff repair (Fig. 22-2). The rotator cuff is first repaired following the technique shown in Chapter 7 through a strap approach. After completion of the cuff repair, attention is turned to the acromion itself, and the unfused epiphysis is exposed (Fig. 22-3). A sliding cortical reverse graft is then fashioned using a small blade power saw. When the graft has been lifted (superficial cortex only), the epiphysial segment is removed using a small dental burr down to bleeding cancellous bone on either side (Fig. 22-4). The two cancellous surfaces are then opposed, and two parallel K wires inserted across the defect.
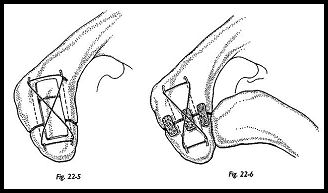
A figure-8 tension band wiring technique is then used (Fig. 22-5). Before putting the final tension on the wire, the reverse graft is then inserted across the epiphysial area, and the figure-8 wire used to hold the graft in place so that the wires cross over the superficial surface of the graft (Fig. 22-6). The ends of the K wires are turned in and tapped into the bone to prevent any superficial irritation.
Alternatively, two parallel Herbert screws may be used to compress the bone across the defect.
Postoperative Management
In the younger age group of athletes unassociated with the rotator cuff defect, passive mobilization only is performed for 3 weeks, followed by active assisted motion for a further 3 weeks, and full active motion at 6 weeks.
In patients with a rotator cuff defect, the aftercare must be tailored to the size of the rotator cuff tear found at the time of operation. Full active movements, however, are not advised until bony union is seen radiographically.
Complications
Complications with acromial epiphysiodesis include problems with the wires. Because of the very superficial location of this procedure, in the thinner patient, the wires may well cause irritation and require removal as soon as bony union is achieved. Another complication is failure to achieve union. It can be difficult to achieve union here, particularly in the elderly with a very thin acromion. However, the procedure described here seems to provide a much more stable fibrous union. Although union may not be achieved symp-tomatically, the patient is usually improved.
Suggested Readings
Neer CS. Shoulder Reconstruction. WB Saunders, Philadelphia, 1990
Neer CS, Bigliani L, Norris TR, Fischer J: The relationship between the unfused acromial epiphysis and subacromial impingement lesions. Orthop Trans 7:138, 1983
