
Preface
THE PREFACES in medical books, particularly in those that concern new fields, are often too brief and impersonal. If an author has conscientiously labored to present his material in clear English, properly punctuated and painstakingly illustrated for the benefit of the reader, surely he deserves to be allowed to indulge himself in his preface. Let him try his sense of humor, however heavy it may be, let him ride his hobbies, relate his favorite anecdotes, tell his life history or otherwise endeavor to please himself. Despise these amusements if you must, but do not forget that they are the normal pleasures of the average man, especially if he is over sixty. No one is obliged to read a preface, but in it the author should introduce himself to the reader and give him a glimpse of his own personality, amusements and intellectual processes. Both author and reader, before they begin any serious study, should enjoy themselves after the example of a pair of interlocking directors beginning their business with some passable golf, a shower, a rubdown, a cocktail, dinner and coffee, before they go to work. These good business men may have heard each other's stories before and may thoroughly distrust one another, but the exercise, the glow, the comfortable, warm, satiated abdominal sensations, predispose not only to digestion but to reasonableness. A preface should produce a similar mutually-forgiving human state of mind, and give the reader and author a certain percentage of trust in one another—of course not complete.
Another advantage of this type of biographic, conversational, light, perhaps flippant preface, might be a chance that the book would be of permanent value, for most medical books are scarcely more enduring than shooting stars, in fact many are obsolete by the time they are published. Hence a preface, serenely, frankly, kindly and even egotistically written by a happy, understanding soul, might preserve a volume through the centuries, although the subject matter of the book might last only a year.
I want egotism in my author or teacher. I want to know what life he has led, what were his aspirations and what are his regrets. Let him be as unconventional as he wishes, but let him refrain from even customary lies and give freely of himself. Things which have become conventionalized like prefaces, funeral services, wedding vows, and legal preambles are to be suspected of evading responsibility. Give me something that is different, for there is a chance of its being better. Voluntarily to be different is to take responsibility and every sentence in an original book might begin with I, for the author only is to be judged.
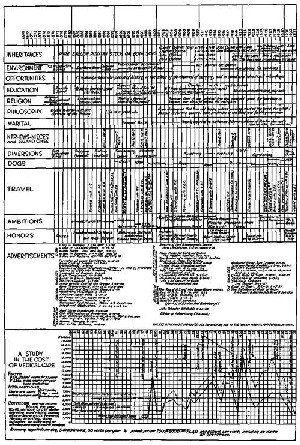
Necessity for economy compels me to reduce my life history to the accompanying chart, and to refrain from describing many incidents which have been exciting and amusing or of absorbing interest to me, personally. It is my intention to comment mainly on those events which concern my work on the shoulder and on what I term the End Result System of Hospital Organization, on propaganda for which I have spent most of my energy, including that expended during the last five years on this book. Meanwhile I have had to earn most of my living and therefore present income curves on the chart to permit me to introduce a necessary part of my thesis, the cost of medical care, a subject that has much to do with Hospital Organization.
I was a conventional enough Boston-Harvard boy, with relatives and acquaintances among the well-to-do, and took two years in the Harvard Medical School with success, and in the third winter had the opportunity to travel in Europe and Egypt with a friend, on the understanding that I could spend as much time as I wished at the Clinics in the various cities we visited, London, Paris, Berlin, Vienna, Cairo and others. This experience and some study on the way enabled me to pass my third-year examinations and to get my degree on my return.
It was in Vienna that my attention was first attracted to the subdeltoid bursa, because it was mentioned in a little book by Dr. E. Albert ("Diagnostik der Chirugischer Krankheiten." Alfred Holder, Wien, 1893). I had never heard this bursa spoken of at home by my teachers, nor do I think it was mentioned in American medical literature at that time. Soon after my return I served two years as surgical interne at the Massachusetts General Hospital in Boston, and during this period, sometimes made diagnoses of subdeltoid bursitis, which were ignored by my seniors. Starting practice in 1895, I became Assistant in Anatomy at the Harvard Medical School, and, for several years, having many opportunities to dissect the bursa and to study its pathology, I gradually came to appreciate its clinical importance. Appointed Surgeon to Out-Patients at the Massachusetts General Hospital (hereinafter M. G. H.) in 1899, I began to have great clinical opportunity, and treated many patients on the diagnosis of bursitis. My first paper mentioning the subject was in April, 1904, although previously at the request of Dr. Mum-ford, then Chairman of the Staff Meetings, I had presented a resume of my work, demonstrating many anatomic specimens and some patients. This attracted the attention of Dr. George Crile of Cleveland, who invited me to read a paper on the subject before the Medical Society of that city. Flattered by this invitation, I wrote a paper with great care and it was well received. During the discussion Dr. Carl A. Hamann of Cleveland mentioned a paper by Kiister published in 1902. I had, at that time, never seen this article, and, though I am frequently quoted as having been the first to describe subdeltoid bursitis, this paper shows clearly that I was not. After seeing Kuster's paper, I adopted his name of subacromial bursitis as better than the term subdeltoid. My work was original so far as I knew at the time, and it was pleasant rather than the reverse, to find that the great surgeon, Kiister, had also thought it worth while to write even a short paper on the subject.
Through much of my life I have suffered somewhat from a sense of isolation, because I have always been thinking, or saying, one thing or another, with which other doctors did not agree. This, in my early years, made me suspect myself of being peculiar, so that, from time to time, I would conform again to general opinions which I knew to be irrational. Even now I have this sense of isolation, although I have become more and more content to wait for acceptance of my views. My regrets are for wasting so much time on the opinions of a previous generation and not realizing that it was the approval of my pupils, rather than of my masters, that was desirable.
When I have given a great deal of study to a subject, I am apt to think I know more about it than those who have not studied it. This confidence probably came because I often stood at the head of my school and yet I have never been able to form very strong opinions on the probable results of races, elections or in futures in the Stock Market, as do many of my friends who were not good scholars. They know whether or not a certain man should be President, whether we should or should not go to war, or even what church to attend, whereas I am in doubt about such things. I am inclined to be impatient with others who do not accept my views on subj ects to which I have given much attention, but if any one else has also given such study and does not agree with me, my confidence in my opinion is readily shaken. Thus, I was greatly pleased to find that Kiister had agreed with me, or I with him, for I was no longer isolated in my opinions. The fact that he had priority was of no significance to me then. I did not realize that it was Kiister who should be pleased because I had sustained his ideas, for now my pleasure comes from having younger men agree to ideas which my contemporaries rejected, or accepted very reluctantly.
It so happened that Rontgen made his announcement of the discovery of the X-ray in December, 1895, at just the time when I started private practice, with the intention of becoming a surgeon. Believing in its importance to surgery, I at once started to learn the technique and sought the help of Professor Trowbridge of Harvard, and also that of Professor Elihu Thomson of the General Electric Company at Lynn. Perhaps it is not generally known that apparatus similar to that with which Rontgen worked had existed for a number of years in many other laboratories. Experiments had been performed to study the effect of electric currents in a vacuum tube invented by Professor Crookes of England. The apparatus had been of great theoretic interest to physicists and was used to produce cathode rays whose paths were chiefly inside the tube. It is said that Rontgen's discovery was accidental because he noticed that a piece of barium-platino-cyanide paper, which happened to be lying on his laboratory table near a Crookes tube, became luminous while the tube was in operation, and that the luminosity stopped immediately when the electric current, passing through the tube, was turned off.
This observation led to his finding that rays, other than those from the cathode, were generated and were projected far beyond the glass walls of the tube. Having noted this essential fact, he went on with a carefully thought-out series of experiments, which demonstrated most of the important points known today in regard to the X-ray. His first paper was a masterpiece. Since every well-equipped physical laboratory already had the apparatus, his experiments were immediately repeated in many places and his conclusions were at once corroborated. Trowbridge and Thomson were among the first in this country to do this, and I had their most kindly, personal, instruction. Having learned the essential points, I found at the laboratory of the Harvard Medical School similar apparatus and began clinical work early in 1896. For five years I devoted most of my time to the X-ray, although still continuing to work in the Surgical Out-Patient Department of the M. G. H. and to assist the late Dr. F. B. Harrington in the practice of surgery. At the end of five years, having written a number of articles on X-ray subjects, including one on X-ray burns, which is still quoted, I saw that I must choose between surgery and rontgenology. An appointment as Out-Patient Surgeon, a title in those days equivalent to that of Assistant Visiting Surgeon, was given me and thereafter my time was devoted chiefly to surgery.
Meantime, 1896 to 1899, experience with the shoulder continued, and in the Anatomic Department I studied the joints and bursae injected with non-radiable material. In 1898, after two years of these anatomic studies, I presented to the Warren Museum an album, which contained standard X-ray anatomic pictures of each joint of the body in flexion, extension, etc. It was a tremendous piece of work, and for me at that time, a very expensive one. Recently, in poking round the Museum, I came across this album covered with dust. It probably had not been opened since left there. However, the experience had been valuable, for, after completing this study of the normal joints, I became interested in their pathology, especially in that of the wrist, knee and shoulder. Furthermore, the fact that my atlas of the normal joints was not used by my colleagues, was a good lesson to my personal sensitiveness and taught me, to some extent, to postpone hope of recognition of labor. A by-product of these anatomic X-ray studies was the light they threw on the normal motions of the wrist joint. These I described in a paper in the Journal of Experimental Medicine. I do not think they had been accurately described before, or have been studied much since. This work led to an interest in fractures of the carpal scaphoid and resulted later in a monograph on the wrist, which has since been recognized.
It would be impossible to give the reader an idea of the thrill experienced by those of us who did the early X-ray work. We each made weekly discoveries, only to find that our fellow workers in the same city and in all other cities had made the same ones at the same time. Announcements of new uses of the X-ray, which are now familiar, came with every issue of the Medical Journals. Each of us had the self-importance to think that we were the first to show fractures of various types, to diagnose bone tumors or to locate foreign bodies in new parts of the anatomy. I remember that an early contribution of mine in the Boston Medical and Surgical Journal was to show that the X-ray was likely to help us in studying the epiphyseal lines! My plate, which was made with a tube which did not focus, after an exposure of over fifteen minutes, showed the epiphyses in the arm of a dead baby. Yet, what I wrote was then unknown to the great majority of readers. We almost forgot that it was all because Rontgen had noticed something which many others might have observed. Probably other things of great importance are showing themselves to us daily, and we look but do not see.
Let any modern Rontgenologist look up my old paper on the wrist, and he will see excellent pictures, taken in 1896, with an old Ruhm-korff coil which Professor Bowditch occasionally used for his physiologic experiments. I remember the Professor's delight when I showed with it, an old bullet in his ulna, which he had carried, without knowing it, for thirty years since the Civil War. Even more delighted was an old lady, who had insisted for sixteen years that she had a needle in her foot, when, after I had located and removed it, she shook it in the face of her doubting family. There were many amusing, exciting and tragic episodes in those days, for we all had burns and some of us gave them. Many of my old friends are now dead from X-ray cancer. It was fortunate for me that my interest in surgery was greater than in Rontgen's discovery.
Side by side with other work, I managed to submit a very extensive monograph for the Gross Prize, which was then given every five years in Philadelphia. The subject was "The Use of the X-ray in the Diagnosis of Bone Diseases." I had collected the histories, pathological reports, X-ray films and end results of cases of bone disease, just as the Registry of Bone Sarcoma does now. There were even examples of such rare diseases as ainhum, chondrodystrophia foetalis, osteogenesis imperfecta and osteoarthropathy pneumonique. With all this material was a resume of the diagnostic points in which the X-ray was of help. The Committee was composed of prominent Philadelphia surgeons, among whom were Dr. W. W. Keen and Dr. J. W. White, and the prize for that year was awarded for an essay on ligation of the carotids in cases of malignant disease of the face! The author claimed that thus starving the growth of tumors by stopping their blood supply was of great help in controlling the disease. The method is now seldom if ever used, yet today, practically everything my paper contained is common knowledge among rontgenologists. It is hardly possible to realize now, that at that time (1905), busy surgeons had no idea of the practical value of the X-ray in the diagnosis of bone diseases, and that the pictures which I presented to this Committee were to them unintelligible!
It was not until five years later, when Dr. Keen asked me to write a chapter on "The Use of the X-ray in Surgery," that I could make up my mind to the shock it gave me to feel that my essay had been discarded, for I felt absolutely sure that it was worthy of the prize. This was my second severe lesson in not being in a hurry about having one's ideas confirmed. However, I had great satisfaction in pulling out from a closet the unpublished paper submitted to Dr. Keen five years before, and, with practically no changes, presenting it to him for his book. Not only most of the illustrations, but the descriptions of the X-ray characteristics of various bone diseases, were from the material submitted for the Gross Prize. The chapter still appears in Keen's Surgery without change.
In 1905-1908 I again worked intensively on the shoulder and published my chief paper which has been so much quoted in the American literature.
We younger surgeons at that time did most of the night emergency operations, and in one such case I was able to make a preoperative diagnosis of perforated duodenal ulcer and to successfully operate on the patient. This took my mind from the shoulder to the duodenum, as it was the first case thus diagnosed and operated on at that hospital. Within a short time afterward, I had several others which were also successful. This led me to study chronic duodenal ulcer, and the shoulder remained displaced behind the duodenum and stomach for the next two years, although my clinical experience with shoulder lesions continued, and unfortunately also, my personal experience as a patient with duodenal ulcer. My chief interest during the next few years was in the surgery of the duodenum. I think I was among the first to appreciate its importance, for I wrote a paper in 1909, when the diagnosis was made so seldom, that I was only able to collect fifty proved instances from our surgical, medical and postmortem records. Of these, eleven were my own cases. I have recently reviewed this paper and was agreeably surprised by the accuracy of the statements as shown by the confirmation of my predictions. However, although working chiefly on the surgery of the stomach and duodenum during this period, I added a point of importance to our practical knowledge of shoulder lesions, namely the demonstration, by actual successful suture of two cases, that ruptured supraspinatus tendons may be repaired. I also drew attention to the importance of examining the patient in a stooping position as an aid to diagnosis in these cases.
Thus, in the year 1910, at the age of forty, I was deeply interested in the surgery of the upper abdomen, still studying lesions of the shoulder, steadfast to my general surgery at the M. G. H., and successful enough to be making a reasonable living in private practice. Then began the great and still unsuccessful interest of my life, over which I have toiled harder and suppressed more regrets, than over any other star-gazing period of my career. Already in 1900 I had become interested in what I have called the End Result Idea, which was merely the common-sense notion that every hospital should follow every patient it treats, long enough to determine whether or not the treatment has been successful, and then to inquire "if not, why not?" with a view to preventing similar failures in future. My chief, Dr. F. B. Harrington, and I had been applying this plan practically to our service since 1900. We had found that this routine tracing of every case, interesting or uninteresting, had brought to our notice many things in which our knowledge, our technique, our organization, our own skill or wisdom, and perhaps even our care and our consciences, needed attention.
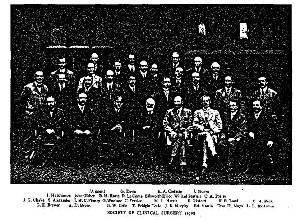
From the day in the summer of 1910 on which Dr. Edward Martin of Philadelphia and I drove back to London in a hansom cab from the Tuberculosis Sanatorium at Frimly, this End Result Idea has taken the major share of my intellectual efforts. Martin at once recognized that the idea was practical, and took advantage of my monomania to make me the servant of his own ideas about Hospital Standardization. We were visiting the British Surgeons as members of a small American Association called the Society of Clinical Surgery.
We had been entertained at a grand dinner by the Royal College of Surgeons, and clinics had been given for us by its various members at the London hospitals. Our little society was composed of very active-minded members, most of whose names are under the accompanying photograph. In this traditional environment, talk of an American College was inevitable among such a group. As far as I know the visit to our British confreres was not arranged for this purpose, but it certainly led to the organization of our American College. If any one, with that idea in mind, arranged that trip, he was certainly the founder, for such men would be sure to go home and found a bigger, if not a better, College. I think that it may have been J. G. Mumford's plan, and that he probably at once talked it over with Cushing, for they were the original founders of the Society of Clinical Surgery. Cushing tells me that he had talked of the question with Ochsner even before this time. I do not know how much had been planned beforehand, but I do know that by the end of that meeting, the American College of Surgeons was under way, even if the method of procedure was not definitely laid out.
Edward Martin, after hearing me discourse on my End Result Idea in the hansom cab, caught at it as the catalyst to crystallize the College Idea. An American College would be a fine thing if it could be the instrument with which to introduce the End Result Idea into the hospitals; in other words to standardize them on a basis of service to the individual patient, as demonstrated by available records. As Martin remarked, "the tail is more important than the dog, but we shall have to have the dog to wag the tail." An American College of Surgeons should be formed to standardize the hospitals, and, when that was done, to continue other good works.
The association with the members of this party, who were not only successful as practical surgeons, but most of whom were connected with teaching or surgical research in our American institutions, was very stimulating to me, although I was only an assistant at home, had never had a hospital service entirely my own, and, owing to the seniority system then in vogue, apparently very unlikely ever to have one. It was also a tremendous stimulus to see the work of the English surgeons, especially that of Mr. Moynihan, at whose clinic I spent several weeks after our official meeting was over. Part of this time I was a patient, and thanks to his skill and a gastrojejunostomy, I was greatly relieved physically, and my zeal for surgery was greatly stimulated mentally. I returned in September, 1910, full of enthusiasm and determined t'o undertake the following things:
First: To proceed with my work on the shoulder, because it was very clear to me that the English surgeons had not yet become interested in subacromial bursitis or in rupture of the supraspinatus tendon. I felt that here was a thing in which, although I could never approximate the contributions of the men with whom I had been associating, I might do my bit, if I could sometime prove in this small matter, that I had added a little to surgical science.
Second: Coming fresh from Mr. Moynihan's Clinic and immensely impressed with his ability to make diagnoses of lesions of the upper abdomen with almost uncanny detail, I wanted the opportunity to demonstrate what he had taught me, and if possible, to progress still further in this kind of work.
Third: More than either of these strictly surgical plans, my talk with Edward Martin and the discussions I had listened to about an American College of Surgeons, took the dominant part in my mind.
I determined that, as any increased opportunity at the M. G. H. was most unlikely since the tradition of a seniority system was so firmly fixed, I would start a small hospital where I would be my own master and could work out my own ideas. I especially wished to make it an example of the End Result Idea. There would be no trustees to consult or other members of the staff to placate, if I wished to state publicly the actual results of the treatment which the patients received. In other words, I would make this small hospital an example of the advantage of an organization based on actual efficiency analyses of the results of treatment.
I set about these plans at once with the result that within a year my hospital was running, and I had two assignments at the M. G. H., one to study shoulder cases, and the other to treat 100 successive cases of ulcers of the stomach and duodenum. I did not succeed in obtaining these assignments without a great deal of trouble, as may be imagined. It was necessary first to convince the rest of the staff that intensive studies of special series of cases were essential for progress, if we were to compete with the large clinics in the neighboring cities where individual surgeons dominated a great deal of material. We had seen the grand old London hospitals being overshadowed by their provincial competitors as an example of such a lack of cooperation. Provided that we each had the spirit to do intensive work on series of cases sufficiently large to make our papers of real value at national meetings, we might still keep our hospital among the foremost in the country and also furnish our community with eminent specialists. Necessarily, if all of our eighteen operators, who shared a service of only 180 beds, were to have a sufficient number of relatively rare cases, each of us must agree to give his major attention to one field.
In search of a convincing argument, I took great pains to look up the end results of our cases of stomach surgery, a total of about 600 in the previous ten years. I tabulated these, not only according to the lesions, but according to the results of each individual operator. These tables offered overwhelming evidence that good results had not been obtained by the eighteen surgeons. There was no chance for discussion, once the facts were reviewed. The rest of the staff, although I was only a junior member, were fair-minded enough to accept the argument and the system of "assignments" was then inaugurated, and still persists at the M. G. H. with the result that some of our operators do have national reputations on the particular lines they have chosen, and yet remain excellent general surgeons. However, I naturally earned by this campaign a certain amount of hard feeling. My colleagues were very glad to have me attend to the shoulder cases, for nobody else was interested in them, nor has anybody selected that specialty since, although it is now twenty-three years since I studied my series of one hundred.
Meantime, I was stressing the End Result Idea and urging the staff and, through them, the trustees, to make our clinic the pioneer in the movement. Through private donations, I obtained the money to provide an "End Result Clerk," whose duty it was to endeavor to trace each patient a year from the date of discharge from the hospital and to enter the result, as noted by the doctor, who had operated, on an End Result Card. I hoped that the M. G. H. might become the example to which to point as a demonstration of the practicability of using this system. It did to a great extent and I was able to use it after the campaign began. (Report of Committee on Standardization of Hospitals. Surg. Gyn, and Obst., Jan., 1914. Not in main volume, but in a supplement on Clinical Congress of Surgeons in back of bound volume, page 7. Another Report of the same Committee appears in the same Journal, 1916, %%: 119.)
I must now digress a little and speak of the Society of Clinical Surgery, which had been in existence a few years before the London meeting in 1910, and was the first of the peripatetic societies organized to meet in different cities to have the members actually demonstrate to one another their operative work and methods of teaching and research. It was undoubtedly the example of this Society which led to the formation by Dr. Franklin Martin of the great meeting of surgeons which came to be known as the Clinical Congress of Surgeons of North America, and which had its first informal meeting in October, 1910, in Chicago. This Congress did not really take shape until the next year in Philadelphia, when Professor Edward Martin was elected President. It met in New York the following year (1912) and Dr. Edward Martin's first act was to appoint two committees; one to organize an American College of Surgeons, with Dr. Franklin Martin as its Chairman; the second, a Committee on Standardization of Hospitals of which I was appointed Chairman, with Dr. W. W. Chipman of Montreal, Dr. J. G. Clarke of Philadelphia, Dr. Allen B. Kanavel of Chicago, and Dr. W. J. Mayo of Rochester, Minn., as the other members of the Committee.
If the subject of the origin of the College ever interests historians, they may be confused as to the parts played by the two Martins. It is at least certain that the then President of the Congress, Dr. Edward Martin of Philadelphia, appointed Dr. Franklin Martin of Chicago to organize the College. Whether Martin of Chicago had previously appointed Martin of Philadelphia as President of the Congress so that he of Philadelphia could appoint him of Chicago to organize the College, I do not know. I do know that the idea of founding the College, to standardize the hospitals, was in embryo in the brain of the Philadelphia Martin two years before this, between Frimly and London. I clearly remember my own feelings, on arriving at this New York meeting in 1912, on being told that I had been appointed Chairman of the Committee on Hospital Standardization, and was to be responsible for the tail to be wagged. This was proof enough for me of the result of my talk in England two years before, with Edward Martin, about the End Result Idea. He had recognized the zealot in me, and had taken this opportunity to thrust on my Puritan conscience the duty to preach the doctrine I had expounded to him. Certainly he also recognized Franklin Martin's ability as an executive, and whoever made the suggestion, chose wisely in appointing him to head the Committee to form the College. Naturally this appointment interrupted my shoulder work, and for eight years my chief thought was to spread the End Result Idea among the surgeons and hospitals of this country. There was, as yet, no authority and little money with which our Committee could work and propaganda was our only means. Since the other members of the Committee were busy men, the chairman had to take the responsibility and get the approval of his Committee afterward. The opening gun was fired at Philadelphia on ~Mny 14, 1913. Edward Martin, by adroit advertising, gathered an enormous audience in the great hall of the Academy of Medicine and I spoke on "The Product of a Hospital." (Surg. Gyn. and Obst., April, 1914, pp. 491-496.) There was much that seemed very radical in tin's address, and the audience showed itself not only interested, but stirred. I asked and discussed such questions as these:
"For whose primary interest is it to have the hospital efficient?
For (1) The patient who seeks relief.
(2) The public who support the hospital and in return expect a high standard of knowledge; on the part of their own private physician or surgeon.
(3) The hospital itself which, as an institution, has an individuality of its own.
Who represents or acts for these interests ?
Strangely enough the answer is: No one; it is for the interest of no one. It is the duty of no one.
For instance: For whose interest is it to investigate what is the actual result to the patient operated on ?
For whose interest is it to insist on the resignation of incompetent old Doctor So-and-So, who is one of the best fellows that ever lived?
Who will warn the largest contributor that his agreeable classmate, Doctor So-and-So, is totally unfitted to remove his stomach ? "
"There is a difference between interest and duty. You do your duty if the work comes to you, but you do not go out of your way to get the work unless it is for your interest.
I>et us make attention to the medical and surgical efficiency of the hospital the duty of some one."
I closed the address with the following suggestions:
"That each prominent hospital in this city appoint an efficiency committee consisting of a trustee, a member of the staff, and a superintendent.
That these committees inquire into the efficiency of their own hospitals with a view to answering the questions which are sure to come from the Carnegie Foundation" (which had just then agreed to help with the movement).
"That an example of this kind set by the Philadelphia hospitals would lead to the establishment of similar committees in other cities, and eventually lead to a national organization representing the patient, the public and the individual institutions."
The surgeons of Pennsylvania rose to the occasion and, under the leadership of Dr. Edward Martin, set a grand example. Dr. Baldy did heroic work, and, for a time, Pennsylvania was the shining light of this new form of hospital housecleaning.
The first report of our Committee was read at the next meeting of the Clinical Congress of Surgeons held in Chicago, November 11, 1913, as was also the report by Dr. Franklin Martin's committee which, thanks to most energetic work on his own part, had organized and incorporated the American College of Surgeons on May 5th of that year. Not until four years after this did the Committee on the Standardization of Hospitals become a committee of the College itself, and hence much more potent than had been our first merely suggestive Committee, whose only authority was the informal Clinical Congress. By 1917, Dr. Franklin Martin had produced a very strong, lusty dog to wag the tail of Hospital Standardization. Moreover, in the sixteen years which have passed since then he has kept that dog in a healthy, hearty condition, in spite of the fact, that the incessant wagging of the tail lias disturbed many slumbering hospital trustees and indolent or inefficient hospital staffs. He has given a most interesting account of the formation of the College in Surg. Gyn. and Obst. (1925, 40: 129), but, perhaps owing to lack of space, he does not mention the work which was done by our Committee during the period prior to 1917, when the cause was unpopular and the College was not strong enough to undertake the expensive practical program.
I think we deserve some credit not only for preparing the minds of those interested in hospitals, but of those who later furnished much of the money with which the work was eventually carried out. I have the greatest admiration for the way in which Dr. Franklin Martin has managed this organization and carried it thus far on its successful career. Nevertheless, although he has actually done the work, it is my opinion that members of the Society of Clinical Surgery, and especially Edward Martin of Philadelphia, helped plan the project and the methods by which it was launched, and have constantly and consistently helped Dr. Franklin Martin by putting their shoulders to the wheel whenever they were wanted. No further proof of this is needed than the public lists of those who have served the College as officers, the great majority of whom have been the members of this small Society.
Dr. Edward Martin is a person who dreads praise more than blame. He has shirked the public responsibility of receiving any kind of praise for the altruistic work he did in the period from 1910 to 1917, until the success of the College became assured. Dr. Franklin Martin has done the hard work and done it well, but the part that Edward Martin took should not be allowed to pass without public mention. I bear witness in this book, because I have given much of my energy through all these years to do what I could for the College according to the ideas which were talked over with Edward Martin on the occasion above mentioned. Perhaps other memoirs than mine may prove whether the Philadelphia Martin, as I think, maneuvered the Chicago Martin into his part in the play, or that the reverse was the case. I am sure that the Philadelphia Martin, taking advantage of my dominant idea and my hereditary Puritan characteristics, made me the servant of his own plans. This is acknowledged in the dedication of the first report of my own hospital. Furthermore, if I had not been working on this plan between 1910 and 1912, I could not have produced the paper entitled "The Product of a Hospital," read in May, 1913, nor could I have produced my "Study on Hospital Efficiency," which was presented in May, 1914, at a meeting of the American Gynecological Society, where it was well received and published in their transactions (Vol. 39) of that year. In this study I was able to use the cases which had been at my own hospital from its opening, August 25, 1911, to July 30, 1913, as a practical example of the operation of the End Result Idea. The correspondence which I conducted during these years has been stored in the Boston Medical Library, in case it may be of interest to some future student of this era. Whatever historians may ultimately conclude, I am personally satisfied that the End Result Idea took an important part in the founding of the College and that this is proved by the first report of our committee in 1913, although the basic suggestions contained in the report have been obscured in the complexity of the record systems later recommended by the College.
During all the time that I was trying to saddle our medical community with the End Result Idea, I do not recall ever hurting any of my colleagues or trying anything more unfair than harmless ridicule. I may have hurt their feelings. If I picked at all on individuals, they were men in high positions such as President Lowell, Dean Bradford, Dr. Washburn and Richard Cabot. I doubt if their feelings were hurt or even their self-esteem. I talked to trustees only through their staffs, the press and my pamphlets. I did not even go behind the backs of the members of the staff of the M. G. H., although a number of the trustees were relatives, personal friends, or members of social clubs to which I belonged. There was one exception — a cousin who was a trustee of another hospital, to whom I used to vent my ideas, but he thought little of them, as cousins usually do of those of their younger cousins, whom they remember as little, freckled-faced boys.
In order to attract the attention of the trustees of the M. G. H., I resigned from the staff in 1914 "as a protest against the seniority system of promotion," which was obviously incompatible with the End Result Idea. On the day on which I received the acceptance of my resignation, I wrote again, asking to be appointed Surgeon-in-Chief on the ground that the results of my treatment of patients at their hospital during the last ten years, had been better than those of other surgeons. I had tabulated my results in case they should ask to see them, but as no one had ever inquired into the results of other surgeons, there was of course nothing with which to compare mine. . Thus, as I had planned, this fact was brought to the notice of the trustees, although at some personal sacrifice on my part. Naturally, my letter was ignored, and I was not appointed Surgeon-in-Chief. However, it was not long before the seniority system was dropped, and a portion of their budget became devoted to a Follow-up System.
It became apparent to me that the medical profession of Boston, its great hospitals and the Harvard Medical School, must be made to pull together with real strength of will, if Boston was to set the example in this movement. Only three great cities in the country were, in my opinion, fitted to take the lead — Boston, Philadelphia and Baltimore — for in each of these cities the majority of the profession were graduates of their respective medical schools and, therefore, there existed in each a certain esprit de corps. Philadelphia, at that time, was a little ahead. It seemed to me that Boston had the best opportunity, for the Harvard influence extended not only through the medical schools and hospitals, but into the banks and into every branch of business, philanthropy or social endeavor. There were two ways open to unite the wills of the various branches of our community, leadership on my part, or a defence-reaction on theirs. Had I the qualities of leadership, I might inspire a band of hard-working lieutenants, and in time succeed in uniting the required number of wills to change any precedent either at Harvard or at its affiliated hospitals. This would be a matter of many years, and I was only a junior surgeon who must also earn his living. I had, on the other hand, observed that the defence reactions of our social forces were fairly prompt and forceful. Harvard is sensitive to ridicule, and also, I sincerely believe, to presentation of facts. If I could awake the steam roller of Harvard public opinion, either by a clear presentation of facts, or by well-advertised ridicule, I felt sure I could get at least a united defence-reaction and some inquiry into existing conditions. I was confident that the End Result Idea would become an intellectual landmark of which any university would be proud, and which, in time, Harvard would claim as a jewel in her crown, and set it with the diamonds of ether anaesthesia and social service.
I was so much influenced by the End Result Idea that I even consulted two friends who were distinguished alienists and put the plain question to them: Am I a victim of a dominant idea because I am willing to make the main object of my life the demonstration of the importance of the simple plan that hospitals should constantly inquire into the results of the treatment of their patients, and modify their organizations when necessary to obtain better results? I received the answer from both alienists that the degree of mental pathology varied with the value of the idea and with the degree of success in making it appreciated. This comforted me somewhat and made the experiment more interesting, for there was some criterion to look forward to as to my own sanity. However, I was a little in the position of the child who prayed, "Now I lay me down to sleep in my little bed; if I die before I wake, how will I know I am dead?"
I admit now that I should have done better to choose either one or the other path and have become a leader or a satirist. I tried to do both and probably lost some time thereby. I tried to run a hospital of my own with an organization to set an example, and at the same time by publishing aggressive reports from this hospital, to apply a little ridicule to Harvard and its affiliated institutions.
As I was Chairman of our local Medical Society in 1914, I took the opportunity to arrange a meeting with the following announcement :
A Meeting for the Discussion of Hospital Efficiency
AT THE BOSTON MEDICAL LIBRARY,
WEDNESDAY, JANUARY 6TH, 1915, AT 8.15 P.M.
UNDER THE AUSPICES OF
THE SURGICAL SECTION OF THE SUFFOLKDISTRICT MEDICAL SOCIETY.
Up to the present time the public and the medical profession have regarded Hospitals as places for the treatment of the sick, but not necessarily for their efficient treatment. Attention has been paid to the cleanliness of institutions, to the architectural arrangement of the buildings, to the kindliness of the staff and nurses, etc., but no attempt has ever been systematically made to determine whether the treatment so freely given has been efficient— that is, as successful as possible.
In most hospitals there has been no official or department whose duty it has been to ascertain the results of treatment at all, much less to compare the results attained by different members of the staff in any one institution, or even to make a collective comparison of the results attained by the whole staff, with those of another similar institution.
Evidently, Trustees, as a rule, have felt that the best they could do was to appoint respectable men on their staffs and then to leave the degree of efficiency of the treatment given the patients to the individual conscience and ability of the physician or surgeon on duty. The terms of duty have been arranged by the calendar or by seniority.
Obviously, if there is any difference in the value of the services of one surgeon or physician and another — which the public seems to admit by its willingness to pay large fees—this difference must be capable of demonstration by some comparative test, so that the distribution of the cases may be made more rationally than by the calendar or by seniority. No physician or surgeon nowadays can be expected to be proficient in all the branches of even a single specialty.
Has the time come when hospital organization can be based on the idea of giving the patients successful and effective treatment as well as care and kindness? Is it possible to compare therapeutic results in medicine and surgery, or must we admit that no matter how much we read, study, practice and take pains, when it comes to a show-down of the results of our treatment, no one could tell the difference between what we have accomplished and results of some genial charlatan or some less painstaking and energetic colleague?
Comparisons are odious, but comparison is necessary in science. Until we freely make therapeutic comparisons, we cannot claim that a given hospital is efficient, for efficiency implies that the results have been looked into. Hospital efficiency is mainly therapeutic efficiency.
The meeting on January 6th is to stimulate thought on these questions. Has it occurred to you that no person or department in a charitable hospital is responsible for the medical and surgical efficiency ?
The speakers will discuss the question of who should be responsible.
The following is the provisional Programme:
Hospital Efficiency from the standpoint of an effiiency expert.
MR. FRANK B. GILBRETH, of Providence, R. I.
Hospital Efficiency from the standpoint of a hospital surgeon.
DR. ROBERT L. DICKINSON, Brooklyn, N. Y., Surgeon
to the Brooklyn Hospital (Gynaecology).
Hospital Efficiency from the standpoint of a hospital superintendent.
DR. HERBERT B. HOWARD, superintendent of Peter Bent Brigham Hospital
Hospital Efficiency from the standpoint of a hospital trutsees.
DR. WALTER WESSELHOEFT, trustee of the Mass. Homeopathic Hospita
DR. JOEL E. GOLDTHWAIT, trustee of the
Robert B. Brigham Hospital.
Hospital Efficiency from the standpoint of a public servant.
His Honor Mayor JAMES M. CURLEY.
General discussion.
E. A. CODMAN, M.D., Chairman.
BETH VINCENT, M.D., Secretary,
29s Beacon Street, Boston.
It was not possible for me to get the proper speakers for this program. I should have had the President of the University, the Dean of the Medical School and the Chairmen of the Trustees of the larger Boston Hospitals. Even some of the leaders of the local profession or representative successful practitioners would have helped. Unfortunately, the President of the University had an engagement for a small social dinner far in advance of the date of the meeting, and so on down the line. Nobody in any position of authority in our medical school cared to take the responsibility of answering these simple direct questions. They all knew that the answer was, that nobody was responsible for examining the results of treatment at hospitals, and that the reason was MONEY; in other words, that the staffs are not paid, and therefore cannot be held accountable. Furthermore, I knew that even the speakers whom I did succeed in obtaining, could not, as guests of our Society, be as frank as perhaps they would like to be, and would not suggest the reason for it, although they might admit the fact that there is no analysis of results in most hospitals.
To make sure that the questions should be answered, I had prepared beforehand, secretly, a cartoon about eight feet long and concealed this under a cover at the back of the stage, ready for use at the end of the discussion, in case no one on the platform or from the audience should dare to suggest the almighty dollar. The large hall in the Medical Library was packed. There was hardly standing room, and the size of the audience was so unusual as to indicate a real desire to hear the questions answered. The presence of the Mayor insured publicity. Moreover, the speakers were interesting and succeeded in sustaining a certain degree of excitement. As my ideas were already known to the majority of the audience, there was an expectant silence, when I rose to close the meeting.
I told of my efforts to get responsible local speakers, how one had a dinner engagement, another was too busy, etc. Then I said that I would present my own answers to the questions in the form of a painting which had kindly been made for me by a friend — the late Philip L. Hale, the artist. No one but Mr. Hale and myself had seen this cartoon, not even the officers of the Society, the secretary of the meeting, or my own wife, who was in the audience. I did not wish any one to share the responsibility for the shock I knew it would give that audience, and I so stated before it was unveiled, with a great flourish, by Mr. Galbraith. The audience held its mouth open while I explained the meaning of the picture, and even after I had finished, continued to be aghast for a minute or two. Then there was as near an uproar as ever I have seen at a Medical Meeting. Some fine old men who had loyally worked for the university, and whose careers I respected, got up and walked out with bowed heads. Other younger ones of the same type rose together to seek the floor, with anger but with nothing practical to say. The great majority, however, were amused more than they were shocked, and a few even risked their reputations by coming publicly forward and shaking hands. For weeks some of my friends did not speak to me, and if I entered a room where other doctors gathered, the party broke up from embarrassment or changed their subject. I was asked to resign as Chairman of the local Medical Society.
For some months I was in disgrace, but the publicity obtained, which spread not only in our local papers but in those of all the other large cities, fulfilled my expectations. My wife and friends had to explain the whole matter daily to other friends, and everybody had to say that what I was after was all right, but my methods were abominable. As nobody else was doing anything about what all admitted was true and important, I had no methods to compare with mine, which did not seem to me either dishonorable or cruel to any one in particular. In a newspaper or in the Lampoon, the cartoon might hardly have been noticed, but at a "scientific" meeting of a Medical Society, attended by the Mayor (although he left after his own speech and did not see the cartoon), it was sure to create the reaction I desired. Soon after, I was dropped from the position of "Instructor in Surgery," which I then held at Harvard. The chart shows the personal financial depression which followed the cartoon, but this did not last long. I had already resigned from the M. G. H. as explained above, and thereafter had only my own hospital for clinical opportunity.
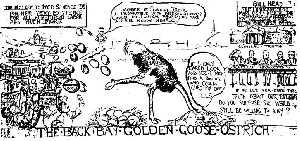
However, I continued my campaign from my hospital, and in 1916 published my third "Study in Hospital Efficiency." This was quite a volume, and since it covered the End Result Reports of five years' work, and also an analysis of all the cases which had died after my operations in fifteen years at the Massachusetts General, it presents ample evidence of the value of efficiency analysis. I sent a copy of this report to every member of the Massachusetts Medical Society and of the American College of Surgeons who would receive one, at a personal expense of about $3,000.00. I still have many copies of this study, one of which I can send to any one who wishes to exchange two dollars for it. I could barely induce people to receive it as a gift at that time, but now I feel that it has a money value. It pleased me greatly that later I had many requests for copies from hospital trustees. In the case of the Woman's Hospital in New York, almost everything that I recommended has been adopted, and I am glad to say improved on, in many details. Several other New York hospitals also accepted the suggestions to some extent. This is evidence that with my sauce of ridicule I served some very solid food for thought. Moreover, in all this campaign I have stood in a glass house while I threw my stones at others, whether they were doctors or trustees. As I did fight from a glass house, I am grateful to them for not destroying me altogether, for, since then, the Harvard Medical School gave me a room for five years from which to conduct the Registry of Bone Sarcoma, and the Massachusetts General Hospital has, since 1929, honored me wit!) the appointment of Consulting Surgeon, which enables me to operate on private patients whom I have referred to its various departments. Still more remarkable than this, the cartoon lias been mounted on cloth, arranged like a folding map, bound and placed for safe keeping in the Boston Medical Library. I publish this cartoon now, because, having been condemned by a previous generation on its account, I hope that I may be judged by a future one to whom the subject will appear less serious. -It depicts President Lowell standing on the Cambridge Bridge, wondering whether it would be possible for the professors of the Medical School to support themselves on their salaries, if they had no opportunity to practice among the rich people of the Back Bay (the residential portion of Boston). The Back Bay is represented as an ostrich with her head in a pile of sand, devouring humbugs and kicking out her golden eggs blindly to the professors, who show more interest in the golden eggs than they do in Medical Science. On the right is the Massachusetts General Hospital with its board of trustees deliberating as to whether, if they really used the End Result System, and let the Back Bay know how many mistakes were made on the hospital patients, she would still be willing to give her golden eggs to support the hospital, and would still employ the members of their staff and thus save the expense of salaries. Across the river and over the hill are seen armies of medical students coming to Harvard because they have heard that the End Result System will be installed in her affiliated hospitals.
A few of my contemporaries have credited me with "moral courage," but I deserve no such credit, for I have merely reacted to stimuli. I may relate, as a parallel, an incident which occurred in 1897 in a part of the country called the Big Horn Basin, then a wild and desolate region. I was traveling with a "pack outfit" when, one day, we met a lone rider with a huge, ugly-looking dog, more like' a mastiff than one of any other breed. The rider was a typical "bad man" who "toted" two guns and was quite as unprepossessing as one of the western villains of the modern movie. He rode along with us for a time and presently we came across a small herd of cattle, loose on the range. The dog made for them and rushing into the herd, "cut out" a cow and a calf, and proceeded to grab the calf by the ear. The bellowing cow made repeated dashes at the dog, but at every rush the dog would swing the calf around so adroitly that the mother butted the calf instead of its enemy. What with the bellowing of the agonized mother, the squealing of the frightened calf and the growling of the dog, it was a noisy and most unpleasant scene. As the owner of the dog did nothing, I dashed up, dismounted, mixed up in the rumpus and kicked the dog with all my might. He crumpled up with a gasp and lay still, so that I thought he was dead until presently he pulled himself up and whimpered off with his tail between his legs. I got away with it, but I was probably in the presence of the greatest danger of my life, not only from the two-gun man and the dog, but especially from the cow. The act was from impulse and was not a product of thought or intention. I simpty could not stand the sight. It was folly, not courage, and the other youth in my party had more sense than I. Our old guide later informed me that the dog was very valuable to its owner, who was a " rustler " and had trained the animal to "cut out" calves and hold them to be branded; but the point I wish to make clear is that my real danger was from the cow, whose cause was also mine.
Whatever credit I may deserve for my tirades should not be for moral courage, but it seems to me that I deserve some credit for restraining myself as well as I have done, having once started on the campaign. To see our hospitals turn their faces away from evident facts is as repulsive to me as to see a calf bullied by a dog, while I stand by and do nothing. What straight-thinking surgeon will deny that on any day at any public hospital one may see suffering, greater than that calf's, caused by incompetence or by neglect of well-known principles of diagnosis or treatment, on the parts of either the physicians who treated the patient before his entrance into the hospital, or those in charge at the hospital. It is not these physicians I attack, but the lack of logical organization in our profession where, as students, we get instruction by example. I am sure I have suffered in greater degree by refraining from saying more about our medical and surgical customs than I have from the professional and social slights received in consequence of saying as much as I have said. If the western scene had been in the center of our Harvard Stadium, and the owner of the dog had been a favorite of the university, imagine what a brute I should have been called! The university, like the poor cow, regarded me as an enemy for trying to remove humbug from its grip on her offspring's ear. However, social position protected me in both instances. On the plains my companions carried guns and our old guide had his rifle across his lap. When I attacked our system of medical education, argument was impossible, for every man in the audience knew that I was right. I had held it naked in the glare of publicity, and the only thing that could be done was to ignore the episode, and to proceed to dress it up a little in case of another flash of lightning. There is now an improvement in the salaries of our professors, who are able to confine themselves more strictly to their teaching and their records, but a thoroughgoing comparative analysis of the results at their affiliated hospitals is not, as yet, a conspicuous feature in their prospectus. They are still obliged by the sentiment of our community to give more publicity to the art than to the science of medicine, while they continue to perform their individual experiments.
When the War broke out I was contentedly carrying out my numerous plans. My friends in the Society of Clinical Surgery, although perhaps also shocked at my methods, were loyal. Even my former comrades at the M. G. H. showed some forbearance and were doing what they could to help. The fellow members of the Committee on Hospital Standardization had signed my reports, although at their own hospitals they were unable to fully exemplify the high ideals which we were recommending to others. By 1917 the American College of Surgeons had taken over the Hospital Standardization work, and it has since flourished under the able leadership of Dr. Mac-Eachern. I was enlarging my little hospital as fast as I could make, or borrow money. The M. G. H. was maintaining its End Result cards; the follow-up system and the special assignment policy were flourishing. Other hospitals were following suit. My operations at hospitals other than my own were supporting me and slowly helping me to expand mine. I heard more and more signs of appreciation of what I was trying to do. I often think that had it not been for the War, my plans would have reached a real fruition, but when War came, the thoughts of men, my own included, left their jobs. My appeals for improvement fell on deaf ears. Most of us worked in the line of our habits, with minds on the War and intellectual processes wandering even from hobbies. No one was interested in avoidable improvements in hospitals or in ideals. Even with my head full of the latter, and although intellectually I could take Germany's point of view, I, too, wanted to volunteer and be with other friends who were joining British units. However, my hospital was holding me fast, and so did my conscience, for I felt I could do more for my country by making a demonstration of the End Result Idea than by doing what other surgeons could do as well in the Army. Conscience is a queer thing in war time. It appears in the hard-boiled and in the ne'er-do-well who have never manifested it before; it makes moral heroes out of some physical cowards and turns some honest men into daring spies or into chivalric aerial murderers. As in peace, we use it to excuse our doings. I regard my own as a troublesome inheritance from my Puritan ancestors which must to some extent be appeased like any other appetite. It is as much a part of me as my foot, although under excitement botli may be forgotten for a time.
Then came the great disaster at Halifax. I telegraphed my good friend, Dr. Thomas Walker of St. John, New Brunswick, offering the help of my hospital staff and a few hours later we were on our way. Dr. H. V. Andrews of Boston fortunately came with us, for he soon demonstrated how a surgeon, who has earned his living in general practice during his early years, can be of more help in such an emergency than any single specialist, for our patients, although for the most part needing surgical care, also presented problems in the whole range of specialties, from obstetrics onwards. We took part in the organization of an emergency hospital, which, when we left two weeks later, was running smoothly with an End Result Card for every patient. Although these cards may now be as scattered as the leaves of the Cumfean sibyl, at the time, they served to keep my finger on every pulse in the hospital and to illustrate the simplicity of installing the plan, even in a city paralyzed by a calamity. One physician told me that in half an hour lie had used all his stock of drugs, and found himself of more use as a man in helping steadily for two days to rescue those still alive who were buried or crushed in wrecks of houses than in his role as a phj'sician.
Having left, with regret, the work in Halifax, where, as Major in the Medical Corps of the Canadian Army, I could have been of real service, and having returned to my hospital purely to try to save money, an indescribable restlessness came over me, until in September, I found myself in our own Medical Corps, wrestling, as Senior Surgeon of the Coast Defences of the Delaware, with the impossible "paper work" of our Army, in the midst of the influenza. Presently, what with patients and enlisted men assigned as orderlies to' care for them, I had more soldiers under me than had the general in command of the three old forts. At the end of mjr endurance, I stood one night in the upper ward of the old hospital in which had been concentrated those whom I judged to be hopeless. My other medical officers were sick abed— even my tireless and capable junior, Captain Ellis, was on that night exhausted. The floor was slippery with bloody sputum; there were no nurses; no petticoats of any kind; no bedpans; no gauze and few medicines; in fact, there was no medical or nursing care. Those that were able lurched to a toilet with the aid of some other soldier who had yesterday been a recruit and now found himself an orderly in this death house, mopping up bloody slime from the floor or cleaning the bed of another boy after he had helped to dump the body and the soiled blankets in a box. I turned and said good-night to those boys who were facing their dangerous duty as bravely as those who fought in the trenches. After a few hours I was able to get up and go on with the "paper work," reporting the numbers of sick and dead, filling out the death certificates, making applications for transfer of insane recruits and otherwise obeying the orders of my competent subordinate, a Sergeant of the Medical Corps. There was no time to test the simplicity of my system of records, but there was necessity for me to learn the use and deficiencies of the Army System.
In November, as Itegimental Surgeon in the Artillery, I had a card for every one of 1,800 men, and enjoyed the new duty of studying how to keep men well, and of getting rid of them when sick. Even the old army sergeant was surprised when I would send for a certain list of men to see whether they still had scabies, or some other minor ailment, and no orders had come for an inspection. He gave me to understand that it was customary to wait until a disease had spread sufficiently to attract some attention from a mysterious medical headquarters, which then issued orders to inspect and report. There was much that was interesting to me about this experience, but as it does not bear on my subject I will merely add that, at this camp in Virginia, after the Armistice, I received an honorary appointment as Fish and Game Officer for the General in Command, and my Christmas leave was spent in camp with daily expeditions after pike and bass, duck, quail, and wild turkey, with my agreeable superior.
In January, 1919, not having applied for discharge, because the need for medical officers seemed greater than before, I was transferred to be Surgeon-in-Chief to the Base Hospital at Camp Taylor, and again had a chance to test the working of my record system. Five hundred hospital beds and some S00 convalescent soldiers in barracks gave an excellent opportunity. An orderly carrying my box of cards attended all visits or operations. The cards were not substituted for the regular records, but served to keep in touch with them when desirable. The senior surgeon of a hospital of 500 beds, if he worked eight hours a day, could give less than one minute to each patient, even if he did no operating or executive work (60 minutes X 8 hours = 480 patients), yet, with the aid of my catalogue and of a good orderly, who has since become Dr. Fraasch, I kept a certain amount of supervision over every patient, operated on many, dressed difficult wounds, and made personal notes on the condition of nearly every soldier at entrance, and again at discharge. At least once a week I inspected each serious wound and often had consultations in the Medical Wards as well. My cards were of the greatest help, for I could talk over his cases with each ward officer as often as seemed desirable. However, I must admit that my day was often longer than eight hours.
In June, 1919, I returned to my closed hospital, in debt, with no borrowing capacity, and somewhat disillusioned as to the possibility of altering the ways of human nature by my intellectual efforts. I had patched up too many fine young men to feel much enthusiasm about keeping the aged and infirm alive, or to listen with any pretense of sympathy to even the nicest lady's description of the daily behavior of her digestion. I determined to be a money-maker, at least until I had paid off my debts, and for two years charged most of my patients three times as much as formerly. My hospital reverted to an apartment house, and for nearly a year I steadfastly abstained from embarking on any new adventures for the benefit of coming generations. Nevertheless, I subtly drifted into the organization of the Registry of Bone Sarcoma, because one of my best patients had a bone tumor. My dream was that this one disease could be used as an example of the inadequacy of our present methods, and that some day the records would serve to demonstrate the value of the End Result System in hospital organization. So far as establishing an undeniable record of our present inefficiency goes, I have succeeded, but even now there is little organized effort to prevent these unfortunate patients from being treated for "rheumatism," until it is too late to save them. I have probably spent more time over this Registry, during the last thirteen years, than the average medical student requires to get his degree, yet, in all this time, I have had the actual care of not more than a half dozen patients with this disease, perhaps less than if I had not written at all on the subject. Many consultations, of course, but the patients are not turned over to me, although one may live next door. What is the reason ?
The hardest thing in my Quixotic career to explain to my colleagues is my plan of free consultation in cases of bone sarcoma. Why spend years studying a subject and then refuse consultation fees? In the first place my object was not to make money, but to illustrate a principle. In 1920 we had, in this country, four eminent authorities on this subj ect, Bloodgood, Coley, Ewing and Mallory, who, by years of study, had amply earned more than they would ever be paid. I doubt if any of them have received three dollars an hour for the time they have spent studying, reading and writing about, lecturing and operating upon, or caring for patients with diseases of the bones. I did not wish them to consider me a competitor, but as a helper, and furthermore I needed their authoritative opinions to establish the Registry. These men became authorities because they had been earnest students and teachers. I believe all of them regard the large fees that may occasionally be paid them by the well-to-do, as merely necessary incidents in their work — a vicarious payment at hourly rates for labor and expense. I have received their cooperation, especially that of Dr. Ewing, who has, even more constantly than the others, been willing to undergo that extreme test of authoritative opinion, a written diagnosis before treatment is undertaken and the eventual result known. This is a real test, not only of knowledge, but of integrity, for necessarily these authorities have voluntarily signed their names to mistakes in diagnosis which may cost life or limb, and, in future, be regarded as evidence of ignorance and even of stupidity, after the results are known and better diagnostic methods have become established. Enough years have already passed for most of us to feel humble.
The second reason was to illustrate how little recompense comes to the true student of difficult medical and surgical fields, except the honors accorded them, if they point a way which others may follow with profit. The public pays the prominent surgeon who amputates the leg, not the scholar who first describes the disease, the practitioner who makes the early diagnosis, nor the pathologist who takes the real responsibility at the exploratory operation and gives the final decision to amputate. The surgeon can do a satisfactory amputation before he graduates as interne, and from that time until the day when his hand is tremulous, bifocals are necessary and his own interne keeps him in hand. One surgeon can amputate practically as well as another, but in 1920 there were not a dozen surgeons in America who had an adequate knowledge of the different varieties of bone tumor, to tell, with reasonable certainty, whether, in a given case, amputation was indicated. Even now, when what knowledge we have has been put in an available form, there are not many who have studied it, and yet any surgeon will consider himself justified in making this decision for a patient, perhaps in consultation with some more prominent surgeon who has little real knowledge but much authority.
I wished to make my knowledge of Bone Sarcoma so conspicuous that my opinion would be acknowledged to be of real value, and by making no charge for consultation, clear myself forever from the imputation that I was advertising for that purpose. On the other hand, if a patient, rich or poor, were referred to me to be treated, I would accept the responsibility and operate or not, as I thought wise, making a moderate charge for the conduct of the case, just as I would in one of appendicitis or of some other condition requiring routine surgical technique and less expert knowledge. Furthermore, I was still somewhat in disgrace at that time, and had no charitable hospital appointment and therefore could care for no really poor patients. I wanted to make this obvious, for the paradox showed that the trustees of hospitals do not appoint their surgeons because of their knowledge. In other words, my attitude would constantly bring up to those surgeons, who happened to have a case of bone sarcoma, the questions: "Have I a right to operate on this case merely to get the fee for amputation when there is another available surgeon who can not only amputate as well, but has also spent years in the study of similar difficult cases and whose advice I may ask with no cost to the patient? Would not this patient prefer the care of the other surgeon if he knew the facts ? Are we doing what is fair by our patients if we let them think that skill in operating or general reputation are more important than knowledge about their diseases?" This was not a policy likely to increase my popularity. I did not wish to become known as a surgeon who had special skill, but I did wish to induce the above train of thought in the minds of my colleagues in order that they might talk about these questions at their clubs.
Bone sarcoma was a particularly good illustration, not only because I had no claim to special success in treatment, but because it is a rare and usually fatal disease in which accurate diagnosis and wise advice as to choice of treatment are far more important than the slight superiority in operative dexterity which any one surgeon may possess above the average. In 1920, blunders in the diagnosis or in the choice of treatment were very common in these cases, but could always be pardoned because the most eminent surgeons made similar ones. I had no claim to preeminence as an operator, but the amount of time I had devoted to the study of the pathology and to tracing the results of treatment, would, if the patients themselves could have known its extent relative to that of the surgeons into whose hands they came, have given them some misgiving. My chief interest in all this work was to show, in epitome, an example of the End Result Idea. Could any hospital, which really aimed to do its best for its cases, permit patients with a rare disease to be cared for by members of its staff, no matter how dexterous, who were not conversant with all attainable knowledge about that disease? What incentive would there be to thoughtful young men to spend years in the study of obscure conditions, if patients with these conditions were to! be assigned, by the ward or by the calendar, to other less studious surgeons who were too busy making money even to read the literature of the subjects?
Of course these ideas of mine are unpopular with the majority of our profession who have spent their lives in the practice of the art of medicine rather than in that of the science, and, being financially successful, are able to influence the trustees of hospitals against an analysis of results. For years they have deceived themselves into thinking that they were giving their services to the hospitals, and comparison of achievements would be, to them, as odious as a comparison of incomes. They know our results are not as brilliant as the public thinks. They cannot understand my attitude of beseeching them, the country over, to make a "show-down" in at least the few cases who have bone tumors. They vaguely, and I think correctly, fear that if we succeeded in collecting complete records of every case of bone sarcoma, the evidence would lead to radical changes in our hospital methods. At present there is only a minority which desires such reforms. All honor to the men who have registered the 1,500 cases so far received; they have truly contributed to science.
And now this book is presented to you as a final illustration of my life work, rather than as a monograph on the shoulder. It offers you an instance of how an apparently trivial injury may fall through the mesh of the loose net of our present system, and how the cost of this leakage is paid by the community in the end. The epilogue will use the same "trivial" lesion to illustrate the need of some form of advertising, in order that patients with rare or little known diseases may promptly reach those doctors who are best qualified to care for them. I propose to show that, twenty-three years ago this lesion had already been accurately described, its symptom-complex clearly recorded and appropriate treatment pointed out, yet, in the hospitals of the world today it will be found that it is often unknown, seldom recognized and rarely successfully treated. This is a state of affairs which could not exist under the End Result System, for no "uninteresting" condition which causes prolonged pain and disability, could be thus neglected. Furthermore, I hope to convince you that the cost to the community of only 100 neglected injuries of this kind would have paid for my own schooling and medical education, added to all the money I have ever inherited or received as professional fees. Hence the little study in the cost of medical care which is shown on my chart.
I have given you an account of efforts rather than of achievements, for much has been attempted that has not been accomplished; even the standardization of hospitals on the basis of End Result analysis and the Registry of Bone Sarcoma are not yet successes. Although my effort on every interest has been largely futile, I have at least worked hard while my wagon was hitched to each star. It is difficult to measure the degree of success one attains in anything, but there may be a law of the Conservation of Human Work, just as there is one of the Conservation of Energy, viz., that if a man labors earnestly for some object, while he may not attain that object, his work will count in some way. The by-products may be more important than the product for which an industry was established. I like to think, for instance, that my End Result Idea had a part in the origin of the American College of Surgeons, and is the basic principle of any rational hospital standardization; that the Registry has helped to diffuse the knowledge of bone sarcoma which Ewing possessed, and that it has also afforded opportunity to the brilliant mind of Kolodny; that the introduction of the policy of Special Assignments has made the Massachusetts General an example to other hospitals, has led to many contributions in difficult fields of surgery, and furnished our community with some true specialists.
And now perhaps this book, in which I advocate a plan that all hospitals make, for a time, a combined study of the shoulder, may lead to some unexpected transformation of my labor. If work is accurate and earnest, I do not believe the amount need be large. Momentum is the product of mass and velocity, and there should be a parallel law that the momentum of one's labor should equal the degree of intellectual accuracy multiplied by the quantity of energy given to it. Rontgen wrote his masterpiece in a few months and the small quantity of work was multiplied by a superlative accuracy, yet his contribution would have been impossible without the momentum of the labor of Crookes and Lenard, who produced the X-rays without observing that they had done so. Only the apex of the projectile was defined by Rontgen, but the momentum of all the work on electricity since that of Galvin and Faraday, sent it in a flash around the world. I would like to make this book so accurate and truthful in every way, that it will greatly multiply the labor it has cost. Its intellectual momentum should be of use somewhere, even if not in the way I plan. It may add to that of a book by Veresaeff, "The Confessions of a Physician," published in 1904 by Frederick A. Stokes Co., New York, and Grant Richards, London.
Have you the impression that you have been listening to a hardworking student who has spent his days and nights, months and years, in the belief that he was anointed to reform his brethren? If so, it is false, for I am no reformer on any principle, but merely because I am naturally disgusted with humbug, self-deception, hypocrisy, smugness, cupidity, and injustice, just as many another may be, who has not been in a position to indulge his prejudices. I believe Don Quixote had a good time, and I have had mine, too. What if we have occasionally attacked windmills? There was the joy of battle. I really have no moral principle beyond trying "to do as I would be done by," "honesty is the best policy," and a few other human maxims.
Although seeing no clear reasons for belief in, or worship of, a deity, and having no expectation of an after-life, I find little intellectual difficulty in explaining to myself a desire to take what is usually called a moral point of view. I am satisfied with recognition of the fact that a happy and satisfactory life is impossible, unless one has the sense of being of service to others. The normal individual cannot evade this conclusion, for heredity from countless generations has given him a tribal instinct to appease.
It is so instinctive to wish to be popular with, rather than despised by one's own generation, that great philosophic effort must be made to satisfy this tribal urge in substituting appreciation after death for present wealth or honor. But if the prophet is confident of the value of his service, he may keep his equanimity in spite of the jeers of his contemporaries. Although the End Result Idea may not achieve its entire fulfillment for several generations, I hope to be as content when dying as any soldier on the battlefield, who, although he may have fought for quite the wrong side, feels the glow of patriotism, or as many an old financial baron, breathing his last in his four-poster, convinced that he has left his children protected from a wicked world. Honors, except those I have thrust on myself, are conspicuously absent on my chart, but I am able to enjoy the hypothesis that I may receive some from a more receptive generation.
Agnosticism has advantages over most creeds. It accepts without thanks, from generation upon generation of ancestors who have painfully perfected it, the wonderful psycho-physical machine we call mind and body. They did not voluntarily perfect this machine on our account, although they may have prayed for our souls as well as their own, during a small time-fraction of their racial existence. We need not thank them, but now that we have come to realize that we shall bequeath similar machines to our progeny, we might do something more and leave them instruction books describing the detail of parts, oiling methods and general care. To my mind, morality is almost synonymous with the degree of wisdom we use in caring for and enjoying the use of these delicate but resistant mechanisms and of the ambitions and desires which came with them. Complete enjoyment of our seventy years of allotted use implies the exercise of all the virtues. We must be moderate and proportionate in driving it, although it has been built with self-regenerating mechanisms to stand the vilest abuse. Its desire for a place in the community is as real as its mechanical wants. For full enjoyment all such needs must be acknowledged. If we become disgusted with the folly of our own generation, we can always employ our machine to do something which we think will make life more enjoyable for a future one. My contribution will be instructions as to how to avoid delay on the road when a certain tendon is broken. But appreciation for such work must be postulated, and this is not easy, although to my mind preferable to the embarrassment of accepting the keys of a great city.
Perhaps most creeds have erred in pointing to the past instead of to the future. Men have sanctified and deified their ancestors, and have even sacrificed themselves and each other to them, but no religion of which I know has pointed to the heaven which might exist on earth, if, neglecting our own souls, we sacrificed for the normal lives of the generations yet to come. Many individuals have done this, but it has never been a creed. Why not deify the supermen we may take part in making? There would be more logic in being burned at the stake as a part of a carefully-conducted series of experiments which would eventually render humanity fireproof, than merely to save our own souls. Even if without going so far as to be martyrs, we all gave up accumulating property, and constantly worked for all the children we shall never see, our own heirs would stand nearly as good a chance as they do at present, so far as I may judge from my own chart. Yet I am not a believer in socialism but in aristocracy. The best are none too good to govern us, and even our wise men, individually, are often gullible in medical or spiritual matters. The world will still be pagan while wealth and energy are devoted to the saving of past and present souls, instead of to the benefit of the race, which is the after-life.
At school I gave more thought to collecting birds' eggs, trapping rabbits, muskrat, mink and skunks, than I did to religious instruction ; and since I have practiced surgery, my attention has been riveted on so managing my life that I could get "days off," during the spring for trout fishing and a month in the fall for partridge and woodcock, that I have given little thought to morals and have substituted reasonable habits. If you are to know me, I may as well admit that I have averaged at least thirty days a year in hunting and fishing. I have tried these things in thirty-six States of the Union, in England, Scotland and Ireland; in Ontario, New Brunswick, Nova Scotia, Quebec, Cape Breton; in Egypt and in Yucatan; and in the case of at least two New England states, in nearly every township. Yet, I have never hit ten ruffed grouse in succession. A few years ago I got six in sequence on different days, and am still hopeful, but as in my professional work, the thing I try to do consummates in something else. In this case, in many friendships. My playmates have varied in character from a godly minister, a great philanthropist, a noble general practitioner, to an outlaw who was a confessed murderer, and several town ne'er-do-wells who were "born in rubber boots." Yet most of them have been men I trusted even in their fish stories.
Perhaps I have sacrificed my success as a distinguished surgeon to these pursuits. I have loved them better than teaching dozing medical students, the pride of amphitheatre dexterity, or the hushed dignity of the consultant at the bedsides of important persons. On many a bright October day I have been glad that my talents as a teacher were not in demand. In the spring when I dig up the first worm in my garden, I say with Hambone: "That old red worm he looks up in my face and say, 'Whar yo' fishing pole?'" Then I get my reward for not being an overworked "Chief of the Surgical Service." In summer as I drift about on some out-of-way pond in my portable boat, watching the cotton wool in the clouds, and momentarily expecting a strike from "a big one," I am grateful that I am not in demand at the bankers' bedsides.
But speaking about that portable boat which has accompanied me to many states and has shared some very happy days, you must hear of the day it was first unpacked. The directions which accompanied it were very detailed and specific; just how to lay the floorboard, the ribs, seats, etc. The last one was something like this: "And now get in, and row out into the pond in the nicest little boat you ever sat in." So I say to the reader: "Now start in and read the best book there is on the human shoulder (it is the only one) and do not fail to note that it shows that only ten neglected cases of the injury, prominently mentioned in its title, may cost our community more than would the distribution of 3,000 copies of this book at $10.00 a copy, preface, epilogue, cartoons and all!
