
Labrum (instability) Classifications
- Silliman and Hawkins classification
- Gleno-humeral translation: Hawkins classification
- Recurrent instability: Neer and Foster classification
- Shoulder instability: Matsen’s classification
- Shoulder instability: Gerber’s classification
- Shoulder instability: Bayley classification
- Anterior-inferior instability: Habermeyer classification
- Posterior Shoulder instability: Ramsey and Klimkiewicz
- Glenoid rim lesions: Bigliani classification
- Hill-Sachs lesion: Arthroscopic classification by Calandra
- Hill-Sachs lesion: Classification by Burkhart and De Beer
- Stages of evolution of labrum /capsule lesions in post traumatic anterior instability: Gleyze and Habermeyer
- Shoulder dysfunction in the overhand throwing athlete: Jobe’s classification
- Arthroscopic classification of labrum / capsule lesions in post-traumatic chronic anterior instability : Boileau
- Scapular Dyskinesis: Kibler Classification
Silliman & Hawkins Classification
Silliman J, Hawkins RJ, CORR ,291:7-19,1993
- Voluntary
- Involuntary:
- Anterior
- Traumatic – Acute / chronic
- Subluxation / dislocation
- Atraumatic – overuse / hyperlaxity
- Posterior
- Traumatic – Acute / chronic
- Subluxation / dislocation
- Atraumatic- overuse / hyperlaxity
- MDI
- Traumatic- Acute / chronic
- Subluxation / dislocation
- Atraumatic- overuse / hyperlaxity
- Anterior
Gleno-humeral Translation: Hawkins
Hawinks R et al, Orthop Trans, 12: 727,1988
Grade 1: 0-25% translation - minimal
Grade 1: 25-50% translation - humeral head translates up to the glenoid rim
Grade 1: > 50% translation - upto the rim and over
![]() Top
Top
Recurrent instability: Neer and Foster classification
Neer II CS, JBJS (A) 62:897-908, 1980
1. Atraumatic - congenital laxity: generalised joint laxity
No labral/ bony changes
ill defined 1st dislocation
2. Traumatic- one major injury: no joint laxity
specific labral/ humeral head/ glenoid lesion
definite injury, needs reduction
3. Acquired- repeated minor events: repeated minor injury
increased joint volume
Labral / bone changes develop late
Threat of MDI
Shoulder instability: Matsen’s classification
Matsen EA et al, Clin Sports Med,10:783-788, 1991
TUBS: Trauma
Unidirectional
Bankart
Surgery
AMBRII: Atraumatic
Multidirectional
Bilateral
Rehabilitation
Inferior capsule and Interval
Shoulder instability: Gerber’s classification
Gerber C et al, CORR, 400:65-76, 2002
Class A: Static Instabilities
Class A1: static superior subluxation
Class A2: static anterior subluxation
Class A3: static posterior subluxation
Class A4: static inferior subluxation
Class B: Dynamic Instabilities
Class B1: chronic locked dislocation of the shoulder
Class B2: Unidirectional instability without hyperlaxity
Class B3: Unidirectional instability with hyperlaxity
Class B4: multidirectional instability without hyperlaxity
Class B5: multidirectional instability with hyperlaxity
Class B6: multidirectional or unidirectional instability with voluntary instability
Class C: Voluntary dislocations
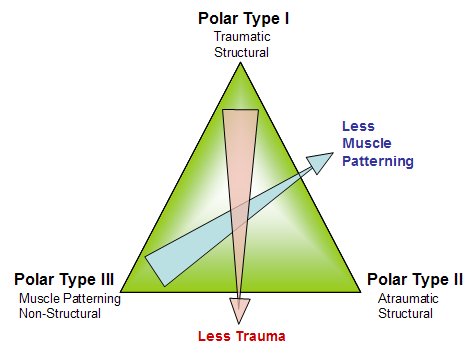
Shoulder instability: Bayley classification
Bayley I, In: The 17th Congress of the European Society for the Surgery of the Shoulder and the Elbow, Germany 2003.
for more information click here
1. Traumatic structural
a. acute
b. persistent
c. recurrent
2. Atraumatic structural
a. recurrent
3. Non-structural (muscle patterning)
a. recurrent
b. persistent
Anterior-inferior instability: Habermeyer classification
In: Schulterchirurgie. Edited by Habermeyer P, 237-271, Urban and Fischer, 2002
1. Bankart line
Classic Bankart lesion
Double labral lesion- labrum detached from glenoid and IGHL
Bony Bankart lesion
2. Perthe’s Line
Classic Perthes- labrum detached from the glenoid rim with IGHL (which is detached sub-periosteally from scapular neck)
ALPSA leion
Triple labral lesion-labrum avulsed from glenoid rim, from IGHL with subperiosteal detachment of IGHL from scapular neck
Extralabral ligament lesion- IGHL avulsed from glenoid, labrum intact
3. Capsular line
Non Bankart lesion- hypoplastic labrum, IGHL inserts on medial scapular neck
Substantial defect of IGHL - intra-ligamentous defects and elongation of IGHL
Quattro labral lesion- avulsion and wear of entire labrum-ligament complex
HAGL lesion- humeral avulsion of IGHL, associated with subscap tears
4. GLAD lesion- chondral lesion at transition zone to labrum, no labral detachment
Posterior Shoulder instability: Ramsey and Klimkiewicz
In: Disorders of the Shoulder: diagnosis and Management. Edited by Iannotti J, 295-319, Lippincott Williams and Wilkins, 1999
1.Posterior dislocation
Acute posterior dislocation
Chronic locked posterior dislocation
2. Recurrent posterior dislocation
Volitional- psychogenic
Dysplastic- glenoid / humeral head retroversion
Acquired - soft tissue / bony deficiency
Glenoid rim lesions: Bigliani classification
Bigliani L U et al, Am J of Sports Med, 26:41-45, 1998
Type 1: united fragment attached to seperated labrum
Type 2: malunited fragment detached from labrum
Type 3A: anterior glenoid deficiency < 25%
Type 3B: anterior glenoid deficiency > 25%
Hill-Sachs lesion: Arthroscopic classification by Calandra
Calandra JJ et al, Arthroscopy, 5:254-257, 1989
Grade 1: defect in articular surface down to, but not including subchondral bone
Grade 2: defect in articular surface including subchondral bone
Grade 3: large defect in subchondral bone
Hill-Sachs lesion: Classification by Burkhart and De Beer
Burkhart SS, De Beer JF, Arthroscopy, 16:677-694, 2000
Engaging Hill Sachs lesion:
lesion that presents its long axis parallel to the anterior glenoid rim in a functional position of 90 deg abduction and external rotation of the shoulder.
Engagement occurs over the anterior rim
Non- Engaging Hill Sachs lesion:
lesion that presents its long axis at a diagonal to the anterior glenoid rim in a functional position of 90 deg abduction and
external rotation of the shoulder.
Lesion passes diagonally across the anterior glenoid thus engagement does not occur
Stages of evolution of labrum / capsule lesions in post traumatic anterior instability: Gleyze and Habermeyer
Habermeyer P et al, JSES, 8: 66-74, 1999
Stage 1: Isolated labrum detachment on a periosteal hinge (Bankart lesion)
Stage 2: Combined IGHL and labral detachment lesion (Perthes lesion)
Stage 3: Triple lesion with degenerative changes of the detached structures
Stage 4: Quadruple lesion- labrum / ligament complex progressively disappears
Shoulder dysfunction in the overhand throwing athlete: Jobe’s classification
Jobe EW et al, Orthop Rev 18: 963-975, 1989
Group 1: -pure impingement
-no instability
Group 2: -Primary instability due to chronic labrum / capsule microtrauma
-Secondary impingement: internal / subacromial
Group 3: -Primary instability due to ligamentous hyperlaxity
-Secondary impingement: internal / subacromial
Group 4: -Primary instability (traumatic)
-no impingement
Arthroscopic classification of labrum / capsule lesions in post-traumatic chronic anterior instability : Boileau
In: Nice Shoulder Course, Edited by Boileau P, 35-46 , Nice, 2003
Labral lesions:
a. Classic bankart lesion
b. Bankart lesion with detachment of superior labrum and biceps anchor
c. Bankart lesion with detachment of posterior labrum
d. Circumferential labrum detachment
e. Absent Bankart lesion
Ligament lesions:
a. Isolated detachment of IGHL from glenoid
b. detachment of IGHL from glenoid with intraligamentous tears; detachment of IGHL from glenoid and humeral side with intra-ligamentous tears
d. Pure intra-ligamentous lesion of the IGHL without glenoid / humeral side detachment
Scapular Dyskinesis: Kibler Classification
Kibler WB et al, J Am Acad of Orthop Surg, 11:142-151, 2003
Type 1: prominent inferior medial scapular border. Motion around transverse axis
Type 2: Prominent entire medial scapular border. Abnormal rotation around vertical axis
Type 3: Prominent superior medial border of scapula, superior translation of entire scapula
